I am vaccinated but I am upvoting this post because I believe that it is important to investigate these cases to determine how to improve future vaccines. I really don't like how this topic seems to be treated like some fringe conspiracy theory. Maybe it is just a conspiracy, but we won't ever know until sufficient research has been done.
Currently, I still believe that people should vaccinate, even if vaccines cause mortality/harm in some cases. As long as vaccine side effects cause less deaths and less harm than the virus, vaccination is still the way to go.
My position depends on us having a good understanding of the vaccine's effects however, and right now I feel like we don't.
The problem here isn't the study---of course we should study possible vaccine side effects. The problem is the massive leaps of logic being made by people who have (quite wrongly, based on available evidence) become convinced that the vaccines are a greater threat to healthy people than the virus is. As unlikely as it is that an otherwise healthy young person will die from covid, it is even less likely that they'll die from a vaccine side effect. That's just a statistical fact at this point, we have millions of both covid cases and vaccinations to back that up.
This study looked at 25 cases of unexpected death in people aged 46-75 and found 5 cases of myocarditis. Without any control group to compare to, there is literally nothing that can be drawn from this study about the risk presented by the vaccine, and the authors admit as much:
"The nature of our autopsy study necessitates that the data are descriptive in quality and does not allow any epidemiological conclusions in terms of incidence or risk estimation."
> The problem is the massive leaps of logic being made by people who have (quite wrongly, based on available evidence) become convinced that the vaccines are a greater threat to healthy people than the virus is.
In some cases, it may well be true that the vaccine is a greater risk than the virus. For example, in Australia, the official recommendation is that healthy people under 30 not receive a fourth dose of COVID-19 vaccine, since Australian health officials believe the risk from vaccine side effects (such as myocarditis) in that age group outweighs the risk of COVID-19 itself. [0] Furthermore, for healthy people in the 30-49 age group, the official Australian position on fourth doses is "permitted but not recommended", since it is unclear if the risk of COVID-19 is greater than that of the vaccine. This is different from the recommendations made by a number of other countries (US, UK, Canada, Singapore), but it appears Australian health authorities weigh the risk of vaccination side effects versus the risk of COVID-19 differently than they do.
Denmark doesn’t recommend COVID vaccines anymore to anyone under 50 who is not at risk or work in health sector [0].
> People aged under 50 are generally not at particularly higher risk of becoming severely ill from covid-19. In addition, younger people aged under 50 are well protected against becoming severely ill from covid-19, as a very large number of them have already been vaccinated and have previously been infected with covid-19, and there is consequently good immunity among this part of the population.
While I think it is certainly fair to talk about the policies of other countries, I don't think just because another country has a different policy necessarily dictates that policy is better or worse.
Additionally, I think it's very easy to see something like "Denmark doesn't recommend the vaccines to anybody under 50" and conflate that it means that Denmark doesn't think vaccines were ever beneficial to people under the age of 50 (which is the leap in logic you often see on anti-vax sites). But that isn't the case. What was good health policy in 2021 is different from good health policy now, because we have way more information about the virus, better and more effective drug to treat it, new variants, etc.
Two things can be true at the same time: The vaccines are
(on net) incredibly beneficial to people and the population as a whole, and yet at the present time there are certain specific populations of people whose optimal number of doses might be fewer than others.
> While I think it is certainly fair to talk about the policies of other countries, I don't think just because another country has a different policy necessarily dictates that policy is better or worse.
Sure. But if a person is aware that other countries have different policies, that gives them a legitimate reason to question whether the policy of their own country is correct. If a person looks into the matter, and decides not to follow the recommendations of their own government, because they think some other country's government is more likely to have got it right, such a person isn't necessarily being irrational/irresponsible/etc, nor would it necessarily be irrational/irresponsible/etc for them to share their conclusion with others.
> and conflate that it means that Denmark doesn't think vaccines were ever beneficial to people under the age of 50 (which is the leap in logic you often see on anti-vax sites)
Yes, many people do seem to conflate these two claims:
(1) "for healthy children and young people, the safety risk of additional doses of the vaccine currently outweighs the risk of COVID-19"
(2) "for healthy children and young people, the safety risk of any dose of the vaccine has always outweighed the risk of COVID-19"
While claim (1) is disputed, some highly respected medical experts agree with it; the same cannot be said for claim (2).
However, I think this conflation goes in both directions – some people who want to defend (2) do so by conflating it with (1); but conversely, some people attack (1) by conflating it with (2).
Some people can't distinguish reasonable scepticism about vaccinations from unreasonable scepticism.
It also is difficult position for health agencies to be in, because they want to make clear guidelines to prevent confusion, but there are gray areas. For example, it's completely possible that:
(a) The benefits outweigh the risks of a 4th shot for any age group
or
(b) The risks outweigh the benefits of a 4th shot for some or all age groups [not because the risk are high, but the benefits so low]
AFAIK, there aren't any super high quality studies anywhere in the world that have robust data on the 4th shot in particular for all age groups. So one health agency might guess one way, another health agency might guess another way. Reasonable people can disagree. The CDC got a little bit ahead of the science when they were initially recommending the 3rd shot, but in the long run it was proven to be a good gamble that no doubt saved thousands of lives. But now maybe that same logic is a mistake for the 4th shot.
But regardless of the CDC's recommendations, most people seem to have figured out the cost/benefit for themselves: The vast majority of people in the US have 2 shots, a little under half have the booster, and very few have the 4th shot. Most people probably have made the right choices for themselves given the various risks and benefits for them personally.
I trust that when I drive over a bridge it won't collapse.
But I cannot say I know that the bridge won't collapse.
Knowledge is a true and justified belief. But trust is not a justification - quite the opposite. If you had a justification, you wouldn't need trust.
Trust whomever you want, on whatever basis you want, but that's fundamentally not reason or rationality, it's just an argument from authority [1]. No statement becomes more true just because someone said it, regardless of who they are.
I'm not saying it's easy or even possible to do in practice. Science is insanely complex. But let's not confuse trust for rationality, not least of which because it brings to the fore the very real need for institutions that are worthy of our trust.
> Trust whomever you want, on whatever basis you want, but that's fundamentally not reason or rationality, it's just an argument from authority [1]. No statement becomes more true just because someone said it, regardless of who they are.
A statement can become more likely to be true just because someone said it, depending on the nature of the statement and the person making it. For example, my brother is an oncologist. If I had some health concern about cancer, I would certainly be asking for his opinion. His opinions on that topic are not guaranteed to be correct, but as an oncologist, they are significantly more likely to be correct than that of the average person.
One problem with the frequent popular invocation of claimed "fallacies", such as "argument from authority", is many of them are only strictly speaking fallacious when used as purely deductive arguments, but real world human reasoning isn't purely deductive, it involves a great deal of induction and abduction as well. There is nothing inherently wrong with an "argument from authority" as an inductive or abductive argument.
> Knowledge is a true and justified belief. But trust is not a justification - quite the opposite. If you had a justification, you wouldn't need trust.
One can estimate the conditional probability P(proposition X is true|agent A says that X is true) based on observations of what kinds of things agent A (or other significantly similar agents) has said in the past, and how many of them turned out to be true or false. You can then use that conditional probability estimate to inform your own decision as to how much credence to give to proposition X. That is both trust and justification.
> One problem with the frequent popular invocation of claimed "fallacies", such as "argument from authority", is many of them are only strictly speaking fallacious when used as purely deductive arguments,
I was not aware of abduction before today, thank you!
I think we may agree in practice if not in theory. I did have the Hume-an problem of induction explicitly on my mind. It would be quite fair to say my epistemology is quite conservative.
Isn't your citing Wikipedia, in itself, an appeal to authority? Why should we accept Wikipedia as an authority on which arguments are fallacious and which are rational?
(Also, that wiki page mentions that many authors don't see it as a fallacy.)
I'm just citing it for the context of the argument both for and against appeal to authority being fallacious and irrational, not that Wikipedia is the final arbiter of what's rational or not. It's more to say that my position is not novel than anything else. Indeed, to be consistent I would need to say that I don't care how many authors do or don't see it as a fallacy :)
You could do some theoretical calculations about bridges yourself, inspect for cracks, and prove from first principles that the bridge is in fact safe; it's not some complicated biological process.
The change in policy by Denmark very likely comes down to the risk of overloading their ICU's with a naive covid population. When covid first arrived everyone was susceptible to covid and the long tail of poor outcomes was enough to plug up the hospitals (and primarily the ICU's).
Now, much of the population has become either naturally or through vaccination much less susceptible to poor outcomes from a covid infection, and this is especially true of younger people.
So the response to covid was never really about the health of the population as much as it was about the health of the hospitals. The risk to the hospitals is now much lower and therefore the reasonable vaccination effort has now changed.
> While I think it is certainly fair to talk about the policies of other countries, I don't think just because another country has a different policy necessarily dictates that policy is better or worse.
Other countries compared to who? Not everyone here is from the same country as you :)
I don't think anyone is making a value judgment based on where the policy is from.
> For example, in Australia, the official recommendation is that healthy people under 30 not receive a fourth dose of COVID-19 vaccine (...)
It should be stressed that this guidance explicitly refers to a fourth dose of a vaccine. I feel it's disingenuous to use this example to try to refute the OP when the problem lies in people taking massive leaps of logic such as going from "it's ok to take 3 doses of a vaccine but the benefits of a fourth might not justify it" to "don't get vaccinated ever because you will die".
> "it's ok to take 3 doses of a vaccine but the benefits of a fourth might not justify it"
That's not what the Australian health authorities are saying. They aren't just saying that "the benefits of a fourth might not justify it", they are saying "(for healthy young people) the health risks of the fourth dose likely outweigh the health benefits"–your rephrasing ignores that safety risk aspect.
In my mind, there are three different positions here:
(1) "Vaccines are perfectly safe, and anyone who even mentions death or serious injury caused by vaccination is just being an alarmist"
(2) "Everyone who took the deadly COVID vax is about to drop dead! Just watch!"
(3) "Vaccines have real safety risks, some people have died from vaccination, and it is certain that more people will die from them in the future. However, sometimes, the risk of death or disability from the disease the vaccine is intended to prevent, is going to be significantly higher than the risk of death or disability from the vaccine. Whether or not that is true in any particular case is going to vary depending on the particular disease, its current prevalence, availability of treatments for it, etc; whether the disease or the vaccine poses the greater health risk will vary across time, place, disease and vaccine; our estimates of those respective risks are always going to be imperfect, evolving, and open to informed disagreement; generally we should trust the public health authorities to make that judgement for us, but they are not infallible, and it can be legitimate to doubt or question their judgement in any particular case"
I see myself as defending (3), whereas what some other people in this conversation are saying seems to me to be closer to (1), and also encouraging the fallacious conflation of (3) with (2).
There is actually a (4) also, which we can see evidence for in a paper such as [1] in the paper Efficacy and effectiveness of covid-19 vaccine - absolute vs. relative risk reduction
Summarized: The Covid vaccines have real safety risks for which there is a body of evidence, that taken in totality, leads one to believe that the temporal and Absolute Risk Reduction of =< 0.85% is not worth the adverse events. Given the suppression of data around the true adverse events, and the time limited protections from the vaccines, it should be used sparingly after the patient is fully informed of the risks, and minimal protections provided. Given the uniqueness of each patient's medical situation though, patients are in the best position to decide if their comorbidities are sufficient to merit the risks of these vaccines. Similarly to the Nordic countries, any younger person without severe comorbidities < 50 should not take the vaccine, but they should be able to make their own decision fully informed of the risks and limited protection, and without any type of coercion.
I don't believe that all Covid vaccines share the same risks since the microgram dosing of the MRNA vaccines vary greatly, and the Novavax vaccine [2] [3] is coming onto the scene, unfortunately with a few of the same adverse events as the MRNA vaccines though
> That's not what the Australian health authorities are saying. They aren't just saying that "the benefits of a fourth might not justify it", they are saying "(for healthy young people) the health risks of the fourth dose likely outweigh the health benefits"–your rephrasing ignores that safety risk aspect.
This is a red herring.
It's irrelevant if anyone feels that the 3rd or 4th or 5th dose of Pfiser's increases health risks. The problem is the misrepresentation of these findings. You cannot in good faith jump from "a residual number of people experience health issues when taking the 4th or 5th dose of Pfiser's vaccine" to "do not take any vaccine at all ever or you'll die" specially when they deny that COVID poses a threat and already killed over 6million people.
You're talking about health concerns of taking a vaccine when not taking the vaccine poses a far greater threat, and somehow that's left out of the equation. That's the problem: the disingenuous misrepresentation of the problem.
I’ve been watching the vaccine discussions on HN these years and one can see that too many people are stuck fighting vaccination windmills from days gone by, while downplaying vaccine risks which by now are established and continue to be investigated as this publication shows.
Meanwhile many EU countries have understood that heart problems are a real risk and have adjusted recommendations accordingly.
They’ve also stopped obsessing about vaccinating people.
The vaccination crusade’s dead folks, please stand by for the next pandemic.
It’s the paradox of intelligence: smart people are more prone to fight tooth and nail, and do all kinds of mental gymnastics, rather than to admit that they too have been misled. People of average or below average intelligence tend to accept it much more easily.
I don’t know if there’s already a name for this phenomenon…
In my experience smart people are also far more likely to create elaborate self-reinforcing systems of belief that are detached from reality.
Any moron can understand the idea of a round Earth and stuff orbiting around it. It takes a genius to comprehend the sublime intricacies of ether vortex theory which explains how a flat Earth can still permit satellites to stay airborne over the plane.
I've met an extremely intelligent person who was convinced we never landed on the Moon and that Stanley Kubrick faked the whole thing and left clues to this in his production of The Shining. I've also met one who thinks the Nazis invented anti-gravity and are hiding the technology to this day in underground bases in Antarctica and South America.
That sounds a lot more like creativity than capacity to reason logically, or a number of other facets of intelligence. That's probably part of the issue, which properties of 'intelligence' we are talking about.
There are also a lot of crazy and intelligent people. I certainly know so many, it almost becomes a correlation.
Were they convinced, or are you convinced that they were convinced? The Kubrick thing is an old joke (which usually ends by saying he insisted on filming "on location" for the sake of authenticity)
I don't either. Personally speaking, after watching the effects of disinformation campaigns over the last 7 or so years -particularly regarding Covid and vaccinations I am pretty much 1,000% unwilling to listen to any "skepticism" simply because I don't trust the source that anyone is getting their information from.
The only reasonable course I can see is to not take any chances and vaccinate early and vaccinate often.
"Misled" is a stupid word for "we constantly learn more and should be adapting our positions."
There is zero evidence for a "haha i told you you were being misled" position. You are performing either foolish or disingenuous logical gymnastics to equate something like "adjusted recommendations accordingly" with "it was intentionally misleading the whole time."
Show me a place where people haven't adjusted their behavior as the virus has evolved, more time has passed creating more data, vaccination rounds have been administered, death rates have evolved, and exposure/infection has happened. It ain't here in liberal California, so is there any such strawman place you're arguing against in the US? Go out on the street and look around and observe that people are being rational and adapting over time instead of keeping up your silly little "haha i'm smarter than you you fell for a hoax" keyboard battle.
Ok, so if you believe your chance of dying of covid is improbably small due to age and overall health, why is it necessary to be vaccinated even if there's only a small chance of side effects? Rare is not zero.
I don't even take OTC pain killers like advil unless I absolutely feel like I have to.
There's also a useful metric for the "chance of dying" - it's known as a micromort. Each micromort is a one in a million chance of dying https://en.wikipedia.org/wiki/Micromort
A fair bit of statistical work has been done on COVID-19 and it is summarized in the wikipedia article.
AstraZeneca vaccination against COVID-19 – 2.9 micromorts[31]
COVID-19 infection at age 10 – 20 micromorts
COVID-19 infection at age 25 – 100 micromorts
COVID-19 infection at age 55 – 4,000 micromorts
COVID-19 infection at age 65 – 14,000 micromorts
COVID-19 infection at age 75 – 46,000 micromorts
COVID-19 infection at age 85 – 150,000 micromorts [32]
Yes, many people survived - but those are not numbers I want to be betting against on a daily basis.
NYT - Putting the Risk of Covid-19 in Perspective
Is the risk of dying from Covid-19 comparable to driving to work every day, skydiving or being a soldier in a war?
> Converting this to micromort language, an individual living in New York City has experienced roughly 50 additional micromorts of risk per day because of Covid-19. That means you were roughly twice as likely to die as you would have been if you were serving in the U.S. armed forces in Afghanistan throughout 2010, a particularly deadly year.
Rare is not zero - but if you are risk adverse, then avoiding things that are fairly high up on the risk counter would be reasonable. Likewise, if there are two options (driving in a car vs driving in a motor cycle), taking the one that adds the least amount of additional risk is reasonable.
We have to be extremely cautious when considering any of the death-related statistics for this particular situation.
For example, we know that a dubious methodology was used for counting deaths in Toronto (Canada's most populous city, and the fourth most populous city in North America).
This was publicly admitted to by Toronto Public Health itself, as early as June 2020:
"Individuals who have died with COVID-19, but not as a result of COVID-19 are included in the case counts for COVID-19 deaths in Toronto."
I can't see how that significant city's death stats could be considered reliable or usable for analytic purposes, after considering how the counting was done. The provincial and national stats would also be affected to some extent.
This makes me quite doubtful about the stats coming out of other regions, too.
The question nobody else has been able to answer is "What is a satisfactory analysis for these purposes?"
The closest I've seen to an answer is to remove accidental deaths (eg, hit by a car, firearms fatality, etc) but there's a huge range of arguable cases like stroke which is plausibly covid-affected. Second, you have the problem of comparing stats between locations that used different definitions, so it's harder to do post-hoc correlations.
The decisions seems to have been avoiding false-negative mistakes by increasing false positives in the first wave of analysis: "Let's include everything under a simple rule for covid stats so that we at least have some kind of worst-case baseline modelling with similar datasets, and we can figure out afterwards which are real and which aren't"
Anyway, just wanted to see if you actually have a better answer to the problem than the standard that was used.
The paper those numbers are based on is Assessing the age specificity of infection fatality rates for COVID-19: systematic review, meta-analysis, and public policy implications https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7721859/
The meta-analysis is looking at that question that you are asking.
It also has all the papers that it cites for analysis and an analysis of its own limitations.
> The systematic review encompassed 113 studies, of which 27 studies (covering 34 geographical locations) satisfied the inclusion criteria and were included in the meta-analysis.
You have to look at both sides of the equation. There are excess deaths in every region coinciding with Covid spikes. It takes enormous mental gymnastics to say “some deaths were over counted so deaths as a whole must be over counted” and completely discount the probability of missing deaths too.
The recent Paxlovid study supports this. It reduces deaths days 30-90. Deaths that would not be counted as Covid deaths. But they clearly are if paxlovid reduces them.
Yeah, it is just wacky stuff for people to be "COVID-19 NBD" while the hospitals are full and the morgues can't keep up with refrigeration requirements... it is not worth engaging with. The exact count doesn't matter, the spikes demonstrate the truth of the issue.
I think that's a pretty specious argument though. Other statistics are available (especially excess deaths) that can pretty clearly help show what was going on along with the COVID death numbers (i.e. a significant increase in the number of people dying through the pandemic who most likely wouldn't have died during that time otherwise, in proportions generally tracking more or less to the reported COVID deaths). It's not like the reported numbers of COVID deaths exist in a vacuum to be able to be so sceptical of them!
> This was publicly admitted to by Toronto Public Health itself, as early as June 2020:
> "Individuals who have died with COVID-19, but not as a result of COVID-19 are included in the case counts for COVID-19 deaths in Toronto."
I don't know the particulars of Toronto Public Health, but this wasn't uncommon for immediate reporting vs death record reporting. Since, in many places, comprehensive death records can take a few weeks (or longer!) to go through the pipeline before ending up on finalized reports, it's useful to have more immediate death reporting during a pandemic. Such immediate reporting is necessarily going to be a little rougher around the edges, but it generally gets you pretty close to the real numbers.
But, it's absolutely true that this immediate reporting isn't perfect. Still, it's very useful, and usually close enough for near term needs. Taking the Toronto example, the main tradeoffs are that a) you include some deaths where Covid wasn't actually a contributing factor and b) you miss deaths where the person was never tested for Covid (especially applicable to deaths that occurred at home). Often, these two somewhat balanced themselves out, but only in places with fairly high levels of testing.
Then, in the medium to longer term, you can switch over to relying on more comprehensive death records. This helps to filter out non-causal scenarios (e.g. the "hit by bus, tested positive for covid, died" scenarios). It also helps add in cases that were initially missed (had symptoms of covid, never went to hospital, died at home, etc).
Finally, to validate numbers, we can also look at excess deaths. This helps ensure that we're not wildly off base with reported numbers. Excess deaths isn't a perfect metric to compare to, but it's still a great benchmark.
To wrap up this comment, let me respond to this:
> We have to be extremely cautious when considering any of the death-related statistics for this particular situation.
I fully agree, but.. I would suggest that your comment missed a lot of the accuracy refinement that happens in practice over the medium to longer term. Additionally, it's very much worth pointing out that, with additional analysis (from death records, from excess death analysis, etc), we've found that very few places were likely over-reporting Covid deaths, but that a significant number of places were under-reporting Covid deaths. So, yes, take shorter term Covid death stats with a grain of salt, but know that we've generally ended up reporting too low, not too high.
> "Converting this to micromort language, an individual living in New York City has experienced roughly 50 additional micromorts of risk per day because of Covid-19. That means you were roughly twice as likely to die as you would have been if you were serving in the U.S. armed forces in Afghanistan throughout 2010, a particularly deadly year."
This is highly misleading. The average individual may be at such risk, just like humans have ~1.9 legs on average, but that doesn't mean that everyone walks around with their 1.9 legs.
So those statistics are based on the risk to the general population and therefore have approximately zero relevance to any single person.
Almost by definition, the disease will claim those most vulnerable first, so questioning whether vaccination is worth it for those less vulnerable is valid.
What're the risks of vaccination vs covid for a healthy 25 year old who works from home?
This exactly. You would want to see the micromort breakdown for the same populations as covid infection. You might also want to dive deeper and see if there's more specific populations and how they compare.
The 50 micromorts per day is from the excess deaths in NYC during spring of 2020 and comparing that mortality to being a soldier in Afghanistan in 2010.
I don't believe that comparing those two is unreasonable.
However, to your last question that is what micomorts can answer.
The risk of death from a vaccination is 2.9 micromorts. The risk of death from contracting Covid-19 for a 25 year old is 100 micromorts. So 30x greater risk.. and those are directly comparable numbers.
The other point to consider - you're not always going to be 25. I'm much closer to the 55 bracket than the 25 bracket, and that represents a 40x increase in risk... so about 1200x greater risk than vaccination.
Assuming you remain a hermit for some number of years (and Covid-19 remains endemic), is there a point where you would change your mind on the value proposition of a vaccination? And if the answer is yes - why not do it now?
Yea, currently you're comparing 2.9 micromorts vs 100 micromorts. At 25, that comparison doesn't have too much to it. 100 micromorts is not something that I think too much about either (comparable to the risk of death while giving birth for the women out there). I've done road trips that racked up 100 micromorts cumulative (more if you add in the hiking and skiing micromorts on that trip).
I'll also note I'm older now than when I was when I did that roadtrip... and there are things that I would do now to further mitigate the risks that I took back then.
It's not wrong for your age, but it is something that should be said "yes, its a risk and it is a lot riskier."
That said, there's a number even beyond that 100 micromorts to consider.
> 1.6 million full-time equivalent workers could be out of work due to long Covid. With 10.6 million unfilled jobs at the time, long Covid potentially accounted for 15% of the labor shortage.
That 4M number is not part that I want to be part of. While I have better than average health insurance, the not-dying also has a significant risk to it too. It is harder to quantify as it isn't an accurate cause of mortality - but it is not something that should be ignored.
Many people here enjoy better than average salaries - consider the risk of going on long term disability for the next 40 to 60 years with the corresponding reduction in compensation. And yes, I know people who are no longer able to work on anything that has a deadline or expectations of attendance in meetings; their lifestyle has changed significantly from three years ago.
> The 50 micromorts per day is from the excess deaths in NYC during spring of 2020 and comparing that mortality to being a soldier in Afghanistan in 2010.
So in other words it's pretty inflated.
1) Putting covid-positive patients in nursing homes instead of isolating them
The by age micromorts are based on a paper that was published in December of 2020. Delta was first detected in the US in Feb of 2021 and named in May of 2021 - again, those numbers are before Delta and Omicron (and vaccination).
The numbers may not be current, but they are not inflated. They are an accurate representation of the excess deaths at that time.
On the scale that micromorts work, that isn't something that it measures well. Micromorts work best for the acute risk "do X and this is your chance of dying." Adding in things that are chronic risks doesn't factor into micromorts well.
Consider "traveling 230 miles by car is 1 micromort"... but that doesn't account for impaired driving or any of the other factors known to influence likelihood or survival of a car crash.
The numbers would likely change if you further specified them, but they are useful for the broad comparisons and risk analysis.
If you've got someone going skydiving every weekend, what does that do to their life insurance rates? Well, skydiving is 8 micromorts per jump. So that's 400 micromorts per year. And that goes into some insurance premium cost calculations.
From Wikipedia:
> Micromorts for future activities can only be rough assessments, as specific circumstances will always have an impact. However, past historical rates of events can be used to provide a ball park, average figure.
Another part of this is a study about risk acceptance.
> An application of micromorts is measuring the value that humans place on risk. For example, a person can consider the amount of money they would be willing to pay to avoid a one-in-a-million chance of death (or conversely, the amount of money they would receive to accept a one-in-a-million chance of death). When offered this situation, people claim a high number. However, when looking at their day-to-day actions (e.g., how much they are willing to pay for safety features on cars), a typical value for a micromort is around $50 (in 2009). This is not to say the $50 valuation should be taken to mean that a human life (1 million micromorts) is valued at $50,000,000. Rather, people are less inclined to spend money after a certain point to increase their safety. This means that analyzing risk using the micromort is more useful when using small risks, not necessarily large ones.
That last sentence is an important one when looking at this.
Would you be willing to be paid $150 to get vaccinated?
Please don't. What you are doing is called "P-hacking". Yes, if you keep selecting for subsets of a dataset you'll eventually find one that, just due to random chance, looks like a statistically significant result that proves whatever it is you want to see. That's not the way you do science.
No that's not P-hacking. The majority of US residents have been infected at this point. The sizes of those population groups both with and without serious pre-existing conditions are so huge that there is minimal chance of an incorrect random result.
Your link is not relevant to this issue so I don't know what point you're trying to make.
To be clear I support vaccination. But patients should make their own decisions free of coercion based on informed consent with full knowledge of the risks on both sides. Don't presume to patronize them with spurious, bad faith comments about "P-hacking". Let's see the actual data.
Right, you have a hypothesis. But you don't have data. Trying to tease out evidence for your hypothesis from existing data by slicing the data set up is the very definition of p-hacking. If you refuse to believe existing work on the basis of an unmeasured hypothesis, well, that's a different sort of logical fallacy on top of the bad statistics.
This is not at all correct. By your definition looking at anything in greater detail is P hacking.
For example, peanut allergies don't exist because most people don't have reactions to them. You absolutely can ask the question for if peanuts are good or bad for a subpopulation.
The alternative is just sticking your head in the sand.
The difference is in the motivations for asking the question and what's done with the answer (so agenda). People are assuming and agenda of others in this thread, and are crafting responses to head of that perceived agenda without actually answering the question, which is rarely productive, IMO. Better to ask than assume, or if the answer is known, provide it with a caveat that it doesn't actually support the specific cases you're worried it might be used for erroneously.
Wrong, I do not have a hypothesis (or any sort of preconceived notion). I am just curious to see what the data shows about risk stratification across age groups with and without common risk factors. Do you have any references to recent peer reviewed studies on that topic?
I'm not sure why you're trying to derail the discussion by bringing up data dredging. That would only potentially be relevant as a possible criticism of the methodology in a particular study. So what's your point?
You didn’t stratify vaccination risk by age which immediately calls into question your comparative data. Indeed the myocarditis risk appears to be inversely correlated with age (exactly the opposite of the positive correlation of risk COVID itself has with age).
These numbers are useless going forward if they are based on the original Covid-19 strains and not the Omicron strains, which now account for virtually every case and are tens of times less lethal.
That's not true. Death rates are now much lower, but that seems to be mostly due to people having (partial) immunity due to vaccination and/or previous infection, and better treatment. Omicron variants are less intrinsically severe than delta, but delta was more intrinsically severe than the earlier variants, so it's not clear omicron's actually any lower than the original strain, alpha, etc.
For example, according to "Challenges in Inferring Intrinsic Severity of the SARS-CoV-2 Omicron Variant" (https://www.nejm.org/doi/full/10.1056/NEJMp2119682?query=fea...): "This meaningful but fairly small difference [vs Delta] implies that omicron, alpha, and wild-type SARS-CoV-2 have similar intrinsic severity."
The argument does not hold water. As Omikron replaced Delta, case mortality reduced immediately, despite skyrocketing cases. Population immunity does not explain this. The figure of 75% is only arrived at by correcting for underascertainment, which is an arbitrary estimate.
Because a) the risk from covid, while small, is still greater than the risk from the vaccines and b) unvaccinated people are more likely to be infected and become a vector for the virus, infecting other people.
Is there any evidence for (b)? My understanding is that you are just as likely to get vaccinated and "shed" the virus for just as long, but are less likely to be severely sick.
Your understanding is wrong. Vaccinated and unvaccinated people with symptomatic COVID shed at comparable rates, but vaccinated people are less likely to get symptomatic COVID. The difference wanes considerably if your last shot was > 6 months ago, but is still present.
> unvaccinated people are more likely to be infected and become a vector for the virus, infecting other people.
I'd add to this the fact that it was especially true earlier in the pandemic, and at that time COVID was significantly more likely to be fatal. Even if someone rejects the idea of getting a fourth dose of the vaccine (rightly or wrongly), it's possible to think that the first two doses were an entirely reasonable one-time intervention into an ongoing pandemic that saved many thousands of lives.
> unvaccinated people are more likely to be infected and become a vector for the virus
I've read conflicting accounts of whether that's true or false, but even if it is - what difference does it make? We're not going to reach heard immunity here. Everybody's going to get it, several times throughout their lives, no matter what we do at this point.
Because the risk of e.g. dying of myocarditis from the virus still exceeds the risk of dying of myocarditis from the vaccine.
Particularly with the mRNA vaccines there isn't much in the vaccine that isn't in the virus already.
There has to be a name for this fallacy. It is like we're living in the dark ages where contracting covid is just "God's will" and it doesn't count in risk assessments, while no matter how small the risk is of the vaccine that is all that matters.
It's definitely not a standard name, but I call kind of reasoning error "active/passive bias": we're generally much more afraid of risks that manifest from action (mauled by a shark while swimming, getting in a car crash) than inaction (dying of obesity, getting hit by a car on the sidewalk).
In the case of COVID-19: you have to actively get the vaccine, meaning that people overweight its risks relative to the risks latent in not getting it.
I think you're right, and an additional factor is that the vaccine is tangible and certain where the virus is invisible and may or may not be present in any given situation (and in unknown quantity).
At its core it may be more that people can't think past binary logic. Either something works or it doesn't work. Either something is perfectly safe or it is too risky. But that doesn't address why they don't apply the same logic to the virus itself (although there are some people on the flip side who still do).
> Particularly with the mRNA vaccines there isn't much in the vaccine that isn't in the virus already.
I don’t find this compelling at all. At the very least, the mRNA vaccines have the lipid nanoparticles themselves, and LNPs are quite clearly biologically active.
And the mRNA gets delivered to cells that would not be infected by the actual virus. One might imagine that such cells would be targeted to at some some extent by CD8+ T cells that learn to recognize spike protein. As far as I can tell, there is nothing published examining what actually happens, but you certainly don’t end up with massive death of muscle cells when vaccinated. See, for example, the comments here:
The lipid nanoparticle itself is basically a cell wall and it fuses with your cell wall and deploys its payload. There isn't a lot there. It isn't like the adenovirus capsid that binds to PF-4 and causes the clotting disorders in J&J and ChAdOx1. It would have to be something related to ALC-0315 and/or ALC-0159 and be active in the very tiny quantities which are administered. Those are lipids and it is most likely that they're eventually just disassembled.
> One might imagine that such cells would be targeted to at some some extent by CD8+ T cells that learn to recognize spike protein.
This is exactly what we want to see happen, and you're going to get CD8+ T-cells from the virus as well (and if you don't, then you're going to get very extremely ill).
The tissue distribution is a reasonably good point, but that should be considered in light of the evidence that the virus itself likes to hide out in places like the gut and that liver and gut activation after vaccination may be protective. And if that argument is wrong, that would be an argument to try to produce nasal mRNA vaccines.
And at this point we do have a really massive amount of data on the safety and efficacy of the mRNA vaccines and we're having to sift the data very closely to find effects lower than one in million. Other vaccines perform worse. I think it probably is because we're getting closer and closer to minimalism.
> This is exactly what we want to see happen, and you're going to get CD8+ T-cells from the virus as well (and if you don't, then you're going to get very extremely ill).
No. What you want to see is protection from the virus, hopefully prevention of infection entirely, hopefully long lasting, hopefully in a form that the virus can’t easily evolve its way out of. And you want this with as little in the way of side effects as practical.
You might think this would happen with an appropriate antibody response or an appropriate CD8+ response or some combination or something else. That’s a hypothesis that may or may not be correct.
But saying that you want your T cells attacking your muscle cells after a vaccine seems absurd. Maybe you can tolerate that (as people apparently can), but I can’t imagine it’s desirable. As far as I can tell, the actual desired means to get CD8+ T cells is for antigen-presenting cells to present pieces of the protein in question attached to MHC1 on their surface, along with the appropriate signals to nearby T cells to encourage them to develop into the right kind of T cell. Your muscle cells are not those antigen presenting cells!
> And at this point we do have a really massive amount of data on the safety and efficacy of the mRNA vaccines … Other vaccines perform worse.
I’m a fan of Covid vaccines too, but this feels like drinking the Kool-Aid. The chickenpox vaccine is effective. The measles vaccine is effective. The tetanus vaccine is pretty effective.
The current crop of monovalent Covid mRNA were highly effective from a week or so after the second dose out to quite a few months against variants closely enough related to the original. [0] Otherwise they are, frankly, far from highly effective. The bivalent vaccines, as far as I can tell, look decent in terms of immunogenicity, but haven’t really been studied well for efficacy against actual infection.
So maybe these mRNA vaccines achieve a form of minimalism, and maybe they’re better than other Covid vaccines, but on the scale of vaccines overall, they’re not great.
[0] Compare to the chickenpox vaccine. In actual randomized trials, they were nearly completely effective even in patients exposed to chickenpox a few days before vaccination. The two-dose series appears to protect recipients for life, or at least decades, strongly enough that epidemic chickenpox is gone in the US. And that continues to work despite chickenpox surely being reintroduced by visitors from abroad on a regular basis and from older infectious shingles patients. That is an effective vaccine.
> Because the risk of e.g. dying of myocarditis from the virus still exceeds the risk of dying of myocarditis from the vaccine.
There's several studies that have shown myocarditis from the virus is indistinguishable from previously-measured myocarditis in the population in general - that the virus isn't actually causing any. At least one of them included vaccine-caused myocarditis and showed it's several times higher.
> People who were infected with COVID-19 before receiving any doses of the COVID-19 vaccines were 11 times more at risk for developing myocarditis during days 1-28 after a COVID-19 positive test.
If we're just going to quote stuff at each other...
> Post COVID-19 infection was not associated with either myocarditis (aHR 1.08; 95% CI 0.45 to 2.56) or pericarditis (aHR 0.53; 95% CI 0.25 to 1.13). We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection.
But also your source is kind of bad. It doesn't have an unvaccinated control group, so from that research there's no way to know if what they found was virus or vaccine related. But they did find an age and sex based correlation which lines up with other sources saying the vaccines are bad for young men:
> The risk of COVID-19 vaccine-associated myocarditis was higher in men younger than age 40 after a first dose of an mRNA vaccine or after a second dose of any of the 3 vaccines.
That isn't relevant because there is no evidence that the vaccine reduces your risk of suffering from myocarditis after infection. (It isn't even necessarily true, but that is a separate matter).
> The risk of COVID-19 infection-related myocarditis risk was cut in half among people infected after vaccination (received at least one dose of a COVID-19 vaccine).
Based on the original strain. Not that I would want to argue. There are several nations that do not recommend vaccination for younger people. They could be wrong of course, but to be so certain about science of a rapidly changing virus and wave away methodological difficulties, like measuring myocarditis without an autopsy, strikes me as scientifically naive, perhaps bordering on religiosity.
With all respect, this is terrible logic. You have two probabilities to compare, not one to compare to zero! If and only if the vaccine is more dangerous then your "improbably small chance of dying of covid", you should forego the vaccination.
Is it? No. It is not. Not even for the best protected youngest cohort. Get your shot. You're being misled by politics and tiny, difficult numbers.
> why is it necessary to be vaccinated even if there's only a small chance of side effects? Rare is not zero.
In my case i vaccinated because i knew i was a transmission node in case of being infected and not noticing, potetially endangering multitude of vulnerable people.
> Because vaccination prevents you from spreading covid to others...
I agree with your general point, but to be clear, it likely reduces your chances of doing that, to some extent. It does not prevent you from spreading COVID.
If vaccination prevents you from catching covid, then it has prevented you from spreading covid to those you would have otherwise.
If vaccination causes you to experience an early immune response, versus several asymptomatic days while unknowingly contagious, then it has prevented you from spreading covid to some of those you would have otherwise.
If vaccination results in a less severe infection with lower viral load, then it has prevented you from spreading covid to some of those you would have otherwise.
My reply was intentionally simple in order to drive home a point about selfish versus societal viewpoints.
> If vaccination prevents you from catching covid, then it has prevented you from spreading covid to those you would have otherwise.
Depends on what you mean by "covid" here. If you're referring to the virus, then no - this is a misconception. The vaccines at best only reduce symptoms, they don't stop infection or transmission.
> versus several asymptomatic days while unknowingly contagious
This was also an early guess that turned out to be wrong. We've known this wasn't a thing for years, at least before these vaccines.
> My reply was intentionally simple in order to drive home a point about selfish versus societal viewpoints.
Right now, getting vaccinated is the selfish action because it's likely to turn you into an asymptomatic spreader. At least when unvaccinated you'll know to stay home.
> Right now, getting vaccinated is the selfish action because it's likely to turn you into an asymptomatic spreader. At least when unvaccinated you'll know to stay home.
This is a) insane and b) directly contradicts the point you tried to make above it.
How does it contradict it? These vaccines reduce symptoms without stopping infection/transmission -> you're helping yourself without helping the community -> it's the selfish action.
> > We've known this wasn't a thing for years, at least before these vaccines.
If I remember the timeline right it was mid/late 2020 we realized that assumption was wrong, then about a year later it was apparent the vaccines weren't stopping the spread. So yeah, my statements are entirely consistent: There wasn't before the vaccines, there was after.
"Not perfect" and "has a small impact" aren't the same. If condoms had the same failure rate in preventing STDs/pregnancy as the COVID vaccines do for preventing infection, we wouldn't use them. Luckily, preventing infection isn't the only goal of vaccines, so it's still worth getting for the protection from severe illness and death.
> If condoms had the same failure rate in preventing STDs/pregnancy as the COVID vaccines do for preventing infection, we wouldn't use them.
No? If they were the best form of contraception we had (which is the relevant comparison w.r.t. vaccines), of course people would use them! It would make abstinence marginally more appealing, of course, but there are already people who don't want or can't afford a pregnancy who unwisely choose to forgo contraception. There would certainly be an enormous number of people who would choose to use condoms rather than forgo sex entirely.
Vaccination has only limited and temporary effects in reducing the risk of transmission. I would encourage everyone eligible to protect themselves by getting vaccinated but this does very little to prevent it from spreading in society.
Spread is just one social effect. I think the GP meant that there are plenty of other civic motivations, like not overloading medical institutions and minimizing the extent to which society needs to be halted to prevent particularly harmful spread.
By all means I would encourage everyone eligible to get vaccinated. But there was never any valid reason to halt society in the first place, so your comment is a non sequitur.
Even before the COVID-19 pandemic, it was routine for medical institutions to be overwhelmed by respiratory viruses. We didn't halt society, we just accepted the consequences and moved on.
There's a significant difference in kind between "a nasty cold or flu season" and the excess mortality rate we've seen during COVID, particularly earlier in the pandemic[1].
There's no non sequitur here: getting vaccinated reduces every demographic's risk of serious illness (even when serious illness is not especially likely!), which in turn reduces the burden on healthcare institutions. That is a good civic reason to get vaccinated that has nothing to do with transmission.
"there was never any valid reason to halt society in the first place"
Look whatever you think about anything full hospitals everywhere and people in Spain being left for dead in old folks homes were definitely real things - I am not sure about your definition of "halt society" here but policy choices that reduced social contact in indoor spaces was absolutely required. You just can't rewrite history if that is what you are trying to imply.
My entire issue actually has nothing to do with health, and everything to do with authoritarianism.
Before the vaccine mandates and coercion I had a seething hatred of corrupt and incompetent little tyrants in positions of power, afterward was nothing new, it just confirmed what I already knew about them. I don't care if I would have a statistically better outcome with the vaccine, I took great pleasure in standing up and defying their bullying and coercion. The wailing and the gnashing of teeth and name calling and crocodile tears from these pathetic clowns about people not getting vaccinated really warmed my heart gave me great pleasure and has mentally helped me tremendously in the past few years. I'm actually starting to feel a bit sad they're slithering back into their holes now, I was hoping for a showdown, but these people are nothing if not cowards like all bullies so this is to be expected.
What surprised me more was how many and how quickly people folded, or never even had any concerns in the first place. Obviously a good portion of the population are a meek and subservient type who want to be ruled and protected. After that a good number are flighty and will panic and run with the heard if something spooks them, sadly a trait that's easily exploited. I really should not have been surprised though, I've seen the same dynamic play out time and time again to start wars, invade privacy, take rights, and take money so irrational optimism that it would be different next time is my failing.
> I don't care if I would have a statistically better outcome with the vaccine, I took great pleasure in standing up and defying their bullying and coercion.
I don't understand this line of reasoning.
If one is being bullied and coerced into what you and I both consider to be the correct decision, one ought to a) make the correct decision, and then b) deal with the bullies?
I don't think I said I considered it to be correct or incorrect, but yes either way I will never take it now. If I had not been bullied by pissant little tyrants I'd have considered getting the vaccine depending on the situation. I don't get yearly flu vaccines either, but I took them in situations that required it (visiting medically sensitive people/places). Not to compare the diseases, just to compare the situation -- I'm also told a yearly flu vaccine is the "correct decision".
But that's really aside, as I said it's not about the clinical benefit of the treatment. I have principles and I have pride, and it would hurt me mentally to do what they tell me. I believe on balance this choice is better for my health. I know several people who didn't want to get the vaccine but were forced to for their jobs, and are deeply upset by that.
I perfectly realize that there are people who get fearful and panicked and are comforted by subservience to authoritarian leaders, who will never understand my line of reasoning. Just like I will never understand theirs. But I can empathize with them -- it must have been terrifying for them, and I don't blame them for being riled up and angry at people who disagreed with them and with their authorities.
What made me sad was how little empathy there has been from people towards what they don't understand. I guess it goes with the fear mindset, fear of the unknown, the other.
> When you admit to making your decision based purely on "seething hatred,"
I didn't "admit" any such thing. My post is there for everybody to read.
> can you really blame people for seeing that decision as irrational?
I don't care what people think of my choices, but I never blamed people or complained about what they think of me. On the contrary I was quite explicit that a large segment of the population sees subservience to authority and following the herd as positive things and can simply never comprehend an objection to authoritarianism or see anything wrong with medical coercion "for the greater good, according to our betters". Clearly they will think my decision is irrational.
> “I drove my car off a cliff to really stick it to society”
Strawman.
> What’s warmed my heart is most Covid deaths being from the unvaccinated. Clearing out the weak and stupid even sooner than natural causes.
And the wailing and gnashing of teeth continues. You sound like a nasty, sick person xcrunner529. They don't make a jab for that.
EDIT: I will give you the benefit of the doubt though, in the spirit of this website. Perhaps you are not naturally like this, but that you have just been radicalized by hateful rhetoric from violent extremists that I see going around all too often these days. And you're lashing out here because you're being precious about the fact you've been lead to believe incorrect things about the vaccines and virus so many times. If that is the case I wish you the best in your recovery.
The vaccine has stayed just as effective for serious disease as it always was said. I am undeniably safer with the vaccine than without as I have actual family members who like you bought into the “vaccine bad” propaganda and died an early death from…COVID.
There really should be real life DARWIN awards.
The great thing, it’s mostly right wing voters dying. :)
> The vaccine has stayed just as effective for serious disease as it always was said.
It wasn't, this is just how you're coping with your cognitive dissonance.
> There really should be real life DARWIN awards.
There are. They are called the Darwin Awards. They have a website and everything.
> The great thing, it’s mostly right wing voters dying. :)
No I know you don't really mean it, you're just angry and lashing out because you've been wrong and humiliated so many times. You're a good person deep down I think.
And surprise surprise, you're wrong about this too. Vaccination rates correlate highly with age, and so do right wing political beliefs.
Because the vaccine is more beneficial for older people. And people can in fact make reasonable decisions about their health. Incredible isn't it?
You put on a brave front, but I think deep down your beliefs don't really comfort you from knowing that you've been fooled and wrong many times, and continue to be. I think and hope you are strong enough to one day come to terms with it though.
As someone who is also fully vaccinated, I am not sure how you can say it is overall good simply because most people will not react poorly. That is like saying Russian Roulette is a perfectly fine game to play because only one person is going to die, and that's OK.
Shouldn't people decide that for themselves?
Note, I am not saying you are saying it is not that they should decide for themselves, it is more that yours is the same logic used to defend vaccine mandates.
Since the Musk takeover, conspiracy theorists on $8Chan have talked about Grant Wahl dying suddenly because of the "clot shot".
Then we find out he died of a ruptured aortic aneurysm.
Then people still refuse to believe it because it doesn't fit their narrative they're pushing. And anyone who dies suddenly must have died because of the vaccine.
The number of doctors who "died" after getting their fourth dose is a moving target, but the article i posted did a bit of a breakdown:
"
The cluster of deaths back in the summer helped kindle what is now a fire — a conspiracy theory that today peddles a list of dozens of doctors online, including the three who died in July, as well as — according to its own descriptions — several who drowned, one who was in the middle of biking 105 kilometres and a doctor who died coming down K2, a mountain deadlier than Everest.
"
It started out as "three" doctors, now it is "dozens".
Are you saying that aneuryms are not a potential adverse event associated with MRNA Covid vaccination [1]?
Furthermore, we know hypertension is also associated with dissections, and there are several documented cases of acute and non-acute hypertension after MRNA covid vaccination [2]
I'm saying that to say there are some possibilities there, but I am also going to say the opposite too.
I don't know that we know enough about the adverse events associated with these vaccinations, and whether or not a vaccine is implicated, or if there was a previous medical condition.
Retrospectively speaking, I don't know that an autopsy would give us any novel answers either, because of the gaps we have around passive medical surveillance vs active medical surveillance.
I am sorry that Mr. Wahl died at such a relatively young age
Actually, this list is insufficient according to the NIH [1] an article in Circulation [2] and my wife, a boarded surgeon. Where she provided data I have italicized it, all others are from NIH and the other source. Interestingly, Diabetes can also have a protective effective against aneuryms [3]. There is also evidence that viral infection can likewise play a contributing role to local inflammation in aorta, similar to the better-known effects of bacterial infections ...CMV infection can stimulate local inflammation in the aorta but is not a direct cause of most abdominal aortic aneurysms. [4]
Genetic/History
Ehlers–Danlos syndrome
Loeys–Dietz syndrome
Marfan syndrome
Turner syndrome
Familial thoracic aortic aneurysms
Bicuspid aortic valve (BAV), which is an abnormal aortic valve
Birth Defect
Diabetes, particularly uncontrolled diabetes
Lifestyle Habits
Aneurysms of blood vessels in other parts of your body
Chronic obstructive pulmonary disease (COPD)
Cardiovascular conditions, such as atherosclerosis, coronary heart disease, and peripheral artery disease
Unhealthy blood cholesterol level
High blood pressure, which is the leading risk factor for thoracic aortic aneurysms but also a risk factor for abdominal aortic aneurysm
Bacterial infections, which are a risk factor for thoracic aortic aneurysms.
Kidney conditions, such as renal failure, chronic kidney disease, and polycystic kidney disease
Obesity
Pheochromocytoma external link , a rare tumors of the adrenal gland that can lead to high blood pressure
Vasculitis
I think a lot of the resentment comes out of "the experts" changing their narratives a dozen times about the efficacy of the vaccines over the last 3 years while browbeating anyone who voiced any amount of skepticism.
"two weeks to flatten the curve", "if you get the vaccine you won't get covid", "the vaccine is 95% effective", "the vaccine is 80% effective", "the vaccine is 50% effective", "well you'll still get covid but you won't spread it to others", "well actually you can spread it to others"
and more... "masks serve no purpose" followed by months if not years coercing everybody into going out with a mask.
But the best one, to me, is when we go back at the very root... "You're a conspiracy theorist like those who believe the moon landing was faked if you don't accept that it's a pure coincidence that the outbreak started in a market next to a lab known to do gain-of-function research on modified bat viruses".
That tune changed too and, at least, discussing the lab leak possibility became acceptable.
It's all seriously WTF. I got two Pfizer shots but I always fought for and respected those who didn't want to get the shot.
And with all the evidence out now and all the countries saying: "We don't recommend a fourth shot if you're below this or that age", I certainly don't plan to ever get a third shot.
Covid was mutating, that's why the advice kept changing. Vaccines were 80% effective, than immune escape happened and the vaccines got less effective. At the same time, covid was getting better at spreading, which is why 2 weeks to flatten the curve wasn't enough.
It's not a bad thing for experts to change their opinion as new evidence comes out.
These people also seem to ignore that CIRCUMSTANCES HAVE CHANGED QUITE A BIT over the entire pandemic. Of COURSE recommendations made when the vaccine first came out might need to be modified or updated as more gets learned about possible side effects and how it interacts with different variants.
These people never seem to have a problem with the changes in the polio vaccine over the years, or chickenpox
It wasn't "science" which was changing its mind though – "science" doesn't have a mind – it was the public health authorities. The same authorities would change their recommendations over time, and authorities in different countries were making different recommendations at the same time. In part, this was due to differences in circumstances (across both time and space) around the severity of the pandemic, availability of vaccines, hospital resources, etc. But, another factor was that, despite (at any given point in time) all having largely the same scientific evidence, they sometimes interpreted it in different ways, drew different conclusions from it, differed in the weight they decided to give to individual pieces of evidence, etc. It is legitimate for people to question whether they were interpreting the available evidence correctly – and this is not just a matter of hindsight, even at the time, there were qualified professionals who disagreed with their judgements.
I think this frequent conflation of "science" with "public health authority interpretations of science" is rather misguided – and it isn't just "anti-vax" people who commit that conflation, many "pro-vax" people do the exact same thing. I've always been supportive of vaccination – indeed, I have all my recommended doses of COVID-19 vaccine – but I think the excessive rhetoric which some people use against those who express doubts has been very harmful – it has actually been a major unnecessary setback in the cause of encouraging vaccination.
People were literally fired from their jobs, removed from 30+ year military careers, over the science, only for the science to keep changing.
If science can't make up its mind and this is "how science works," anyone who thinks anything should be mandated based on science should be shot. You can't tell people something, have it directly and deeply affect their personal lives, then tell them something substantially different 2 years later, without people grabbing pitchforks. Your theoretical definition of science is irrelevant and makes popular perception of "science" a whimsical joke.
The military isn't a good example because they already have mandatory vaccines and those were completely supported, it wasn't until the fairly recent anti-vaccine drama (autism/mercury) mixed with the distrust of the establishment promoted by Trump, that military people (or right-wing media) began to turn this into an issue that people cared about.
> that military people (or right-wing media) began to turn this into an issue that people cared about
Historically, the majority of opposition to vaccines has been "left-wing" rather than "right-wing". It was only really with COVID that it suddenly picked up on the right as well. I've had some rather frustrating conversations online with people (mostly Americans it seems) who are utterly convinced that it is fundamentally a "right-wing" phenomenon, and seem to just want to ignore the evidence of its long history among self-identified "progressives":
I am not aware of what was the case historically (roughly before I was vaccinated as a kid), but I will point out the switch happened before covid- around 2015- and was fairly partisan. Note that extreme idealogies sort of "wrap around" the political spectrum- another area with extremely low vax rates for some time was Marin, which is highly educated and liberal.
I wonder to what extent any "partisan switch" is primarily a US thing? Here in Australia, while some right-leaning people (especially the "hard" right) have in recent years become "anti-vaccine", I haven't seen any comparable evidence of traditional left-leaning "anti-vaccine" adherents abandoning it
I can think of two people my wife and I know personally who are vocally "anti-vax" – one is a rather conservative Christian, the other is a woman with a long-standing interest in the New Age / Tarot / occult / crystals / psychics / alternative medicine / etc. The first, when we were younger (15–20 years ago), I used to run in his circles a lot, and I never heard anybody say anything remotely against vaccines at any of the churches / youth groups / bible studies / etc we used to attend together. He only started becoming "anti-vax" around when COVID started, and it obviously had a lot to do with US politics (he was a big Trump fan, and so was his church–I'm not sure if they still feel the same way about him now), despite living on the other side of the planet. Even then, he was always primarily "anti-COVID vax" rather than "anti-vax" in general.
Our "New Age" friend, her being "anti-vax" was entirely expected, because "anti-vax" opinions have always been very common among people like her. She became very political about it around COVID, organising protests, etc. It became even more intense when she lost her government job (as an adult vocational education teacher) due to her refusal to be vaccinated against COVID. But, the anti-vax protest movement she became involved in was rather left-leaning, it was all composed of New Age types, hippies, etc, who live in a "hippy area" (the Northern Rivers district of New South Wales). I think if someone like our other friend – a conservative Christian spouting pro-Trump rhetoric – had turned up at one of her protests, she would have run them off.
> Note that extreme idealogies sort of "wrap around" the political spectrum
I don't know if that's really true though. While opposition to COVID vaccination may be one of the very few things these two friends of ours could agree on, I think their reasons for their respective positions are very different. I'm not sure the whole "wrap around" or "horseshoe" thesis is really that useful in understanding why two people from opposite ends of the political spectrum may occasionally end up agreeing on something, even something outside the mainstream.
It's not an unreasonable position, or lacking in common sense, to insist that any new drug, particularly one using new technology that has not been used before, have more than one year of testing before it is made mandatory, regardless of the assurances of scientists.
Furthermore, entering the military requires accepting a predefined list of vaccines and that is understood when entering - but adding new vaccines requires following the USC Code, which if you read, I can fully understand why some would feel very uncomfortable with it, and may feel that their protections against being "guinea pigs" have been ran around, as the USC Code would imply that this should not have happened so easily.
Furthermore, not only did we learn more, but the virus itself mutated substantially over time. There were different efficacy rates given in large part because there were literally different vaccine efficacy rates for different strains of the virus.
> The problem is the massive leaps of logic being made by people who have (quite wrongly, based on available evidence) become convinced that the vaccines are a greater threat to healthy people than the virus is.
That may be true overall (and it may not btw, only time will tell), but it's certainly not true on a by-indvidual basis. Someone who's, say, 18 with no major health disorders is going to experience a lot more risk of adverse outcome from any of the vaccines than from SARS-CoV-2. That's partially a function of the incredible SARS-CoV-2 outcomes in the "not old" age range but also because vaccination is also a fundamentally different intervention than exposure to the entire SARS-CoV-2 virus. If we're talking about the mRNA vaccines (Pfizer/moderna/etc), those are basically spike protein mRNA suspended in lipid nanoparticles. It makes your cells express the spike protein, not the whole SARS-CoV-2 virus. So metaphorically speaking you're getting pure spike protein antigen, and different peoples' genetic predispositions/etc are going to play out differently in that scenario as opposed to contact with the normal virus.
...Like those of the people in the case report we're looking at.
You literally just made the wild leap of logic the parent comment was talking about.
The mRNA vaccines have a modified spike protein, that is non functional compared to natural infection. On top of that, cells naturally infected with covid also express the spike protein [1], and would do so in far greater amounts than what would be caused by the vaccine.
People's different genetic dispositions will change their immune response, and that might maybe change how they respond to the vaccine as opposed to the virus. But there's no way of knowing which way you will fall, and our current evidence suggests that getting the vaccine is probably always the safer alternative.
> even less likely that they'll die from a vaccine side effect
My understanding is that there've always been risks associated with vaccines, and they were always relatively small risks. What I can't find any unbiased information about is how the risks of the Covid vaccine compare with the risks of, say, the mumps or rubella vaccines.
Your graph does clearly have a peak at the 2020/2021 boundary, that falls down after the vaccines got widespread, by the middle of 2021 (with most countries going into negative excess deaths). There is another, smaller peak at the end of 2021, that's when omicron got widespread.
This chart isn’t absolute death: it’s the ratio of two causes of death.
You’re not seeing countries go into negative excess in 2021 and 2022 — you’re seeing non-COVID excess surge.
I was expecting during the omicron wave that we had more than two COVID deaths compared to non-COVID excess deaths — and that more broadly, we’d see more COVID than other excess death
What we see instead is that during the height of omicron, 33% of the excess death was non-COVID — and that for most of 2021 and 2022, 66% of the excess death was non-COVID.
What has been killing as many people as a global pandemic? — and if there’s so many non-COVID excess deaths, did our policies help?
When that ratio turns negative, it literally means that there has been negative excess deaths when compared to the average. You can claim that the average is abnormally high, but that's quite a wild claim.
Negative excess deaths through the pandemics were pretty common and very well explained.
Anyway, such concepts like "non-COVID excess" doesn't even start to make sense. Either you are determining the death causes, or you are doing statistical analysis over unknown causes.
When that chart turns negative, it means that the ratio of COVID deaths to non-COVID excess is less than one, ie there is more non-COVID excess death than COVID deaths. When there is no non-COVID excess, but still COVID deaths, the chart shoots up; when there’s none of either, it clamps to the black line. This is a log-scale chart of their ratio; that solid black line represents a ratio of 1, ie, equal amounts.
The chart going below the black line represents positive excess death in a ratio that favors non-COVID excess deaths.
Edit: I’ve added a log chart of excess deaths, with the black line at zero, ie, the expected amount.
> concepts like "non-COVID excess" doesn't even start to make sense
Sure they do: excess deaths which exceed the number of registered COVID deaths in the same period. We can detect that by looking at all cause mortality and subtracting identified COVID mortality.
why is that logic jump is happening? Mostly because of censorship. If your logic needs censorship to prevent logic jumps, perhaps your logic isn't solid to begin with (or mixed with lies like the vaccine).
For healthy persons in certain age group, COVID risk is almost missing. If they don't want vaccine, regardless of taking 3 doses, I have no right to tell them to take not-thoroughly tested vaccine to help reduce the spread at the potential cost of their own.
The solution is more open studies and acknowledge statistical (in)significance of vax side effects instead of trying to shove it under conspiracy and censorship. Oh, and dont lie about vaccine effectiveness.
> we have millions of both covid cases and vaccinations to back that up.
This study looked at 25 cases of unexpected death in
Fair enough, but where is that data? Why a study of only 25 if there are millions?
It's not a conspiracy theory to say such things simply don't add up. The largest drug test in history and no encompassing and definitive follow up? Why?
Many other people have replied with great information, but I'm going to respectfully disagree with:
> The problem is the massive leaps of logic being made by people who have (quite wrongly, based on available evidence) become convinced that the vaccines are a greater threat to healthy people than the virus is.
I believe the problem is that we were so convinced that our solution to covid was infallible that we removed a basic human right: the ability to make informed choice about your medical care.
I'm not a conspiracy theorist, I believe that most people involved did this out of a genuine desire to save lives and help people.
The issue is the hubris.
The idea that "I know better than you do what's good for you and for society, so I'm going to force you to do a thing".
This is where we went wrong. The forcing.
If we'd presented vaccination as informed choice, had recommendations but not coercion, I think there would have been a lot less resistance.
We decided that public health was a trump card that allowed us to ignore almost every civil liberty the U.S. was founded on.
We actively limited speech and debate, going to far as to silence and destroy the lives and careers of qualified physicians who dissented.
We restricted freedom of assembly.
We seized property through forced business closing without compensation.
We restricted free movement.
We coerced vaccination in the strongest possible ways shy of physical force.
The list goes on.
We did this out of a hubris that "we know better than you".
It doesn't really matter whether this is true or not, it's fundamentally anti-liberal.
It's made worse by the unfortunate fact that in most cases we were wrong.
Asymptomatic spread wasn't a thing. The initial studies that said it was were based on flawed methodology. Even China isn't counting asymptomatic cases anymore.
Pretty much every model that we based policy off of, predicting extreme fatality rates and recommending extraordinary interventions, were dead wrong.
As others have pointed out, mortality counts were wildly off due to many factors, including how death certificates were filled out (died with covid v/s died from covid).
The vulnerable populations were identified fairly early on, but we chose to implement draconian restrictions for everyone, regardless of their individual risk.
I couldnt have written that any better.
And THIS is why thousands of people showed up in downtown Ottawa and stayed for three weeks. Because we were disgusted and DEEPLY offended by the hubris.
And what was the gov's response? An even greater swing toward authoritarianism - the Canadian government literally locked people out of their own bank accounts, seized property and arrested and charged hundreds.
Incredible. Absolutely incredible. The anger is still palpable. And its going to simmer til our current gov is replaced.
> If we'd presented vaccination as informed choice, had recommendations but not coercion, I think there would have been a lot less resistance.
Honestly, I seriously doubt it. I think the resistance would have been about the same; even the most gentle "recommendation" would have been cast as coercive by those who oppose the vaccine now. All a more "gentle" approach would have done is to dissuade those on the fence.
<IMHO>Pharma could go on with huge gains, just selling immunity boosters, like C, D vits, exposing to solar flares... But boosted with 'media', they were forced to take an "social" experiment. Instead, they even forbid going out, and in my town police chased couples sitting on the park bench!! MAdnESs!! My lungs and 55+ sorts me under vulnerables. Even my doctor argued, freightening me, explaining weak immunity, in spite of mentioned immunity boosters my mamma told me to take :) ! At the end my covid experience is funny - weak flu - good to stay at home - want one again!
Divide and Conquer policy, don't you see?</IMHO>
> As others have pointed out, mortality counts were wildly off due to many factors, including how death certificates were filled out (died with covid v/s died from covid).
This has never really been shown to be that accurate considering the excess deaths from the averages every year. You’re ignoring an inconvenient fact.
I took screen shots almost daily of all-cause mortality stats through the lockdown.
The entire time it tracked pretty close to the expected linear increase that we see year over year with an aging population, with the exception of a bump in April that was almost exclusively New York City. Given the reported quality of care issues that drove a lot of that, there are still a lot of unanswered questions.
I also saw a sudden jump in these numbers right at the end of the year. Could have been completely legitimate due to delays in reporting, but for some reason the CDC refuses to release anonymized data sets that would allow independent analysis.
Which is highly abnormal.
Additionally, all-cause mortality measures don't do a good job of indicating covid deaths, necessarily. Many deaths were due to delays of care for critical conditions. I experienced this myself, and was fortunate to not have become a statistic. We had deaths of despair, and we have several conflicting studies about those. We also have a significant (maybe majority) number of the deaths attributed to covid being a six to twelve month acceleration of death for those who were at end of life, especially the elderly with comorbidities.
While sad, it's not quite the terrifying tragedy that the numbers without nuance present. It will be interesting to see if 2022 and 2023 see a concomitant dip in expected mortality.
I also spent countless hours hunting down source data (as much as was available) understanding how Covid ID was generated for cross region case tracking, data collection methodology and evaluting transmission studies and models.
I saw massive revisions of numbers post-investigation in several counties, such as Collin county in TX.
If there's one thing we know for sure, it's that the data is a collosal mess. If you spend any time digging into the data collection methods and how reporting was happening you'd see this for yourself.
FWIW, my background is in healthcare logistics, data analysis and technology.
So if you are aware of some facts that I'm ignoring, I'd love to understand them.
When you've spent the time that I have looking into the source and methodology behind that data, rather than just spending 30 seconds googling, please let me know.
But here, I'll save you some time. Those pretty graphs you're linking to use the HMD database as the primary source through Feb 2021.
Take a look at how the HMD database derives it's numbers [1].
Now we can discuss the issue in rational, educated terms.
Expected deaths for a given year are based on a combination of factors such as the population age, and function fitting previous trends. It would have been around 2.9 million for 2020.
So the raw excess death count for 2020 is somewhere south of 500k.
Many of these deaths were due to covid directly. The vast majority of which were people already at end of life, very elderly and with significant comorbidities.
We're still doing research on how many of these excess deaths were due to downstream effects of covid interventions, such as lack of access to care, deaths of despair, etc...
Also, when researching all cause mortality in 2020 and 2021 make sure to take into account fentanyl, which has exploded during those years and account for over 100,000 deaths in 2021 alone.
There is a lot of evidence that the system to report vaccine injuries is largely ignored and people that report issues are ostracized for doing so. It also begs to question how often injuries would go unreported or misreported because of the difficulties of being linked to the actual cause, and many doctors may be unwilling to claim a vaccine caused an injury just due to the stigma around vaccine injuries, especially in regards to COVID-19.
We've banned this account for using HN primarily for ideological battle. You can't do that here, and yes that rule holds regardless of which ideology you're battling for or against. It's not what this site is for, and destroys what it is for. Please don't create accounts to break HN's rules with.
This paper doesn't claim that mRNA vaccines are dangerous, it investigates through autopsy 35 people in a region of Germany who died within 20 days of vaccination and only 5 of the deaths are found to show myocarditis of which only 3 somewhat might be attributed to the vaccine.
This is not an expose of big Pharma or anything like that, I don't know why the HN comments are acting as if this is some kind of research supporting the anti vaxxer claims.
If you look into the statistics, it actually might be the case that those 35 deaths were attributed to the vaccine. They found for fact that 10 of those died actually died of something else.
This is also why it takes an expert in a field to evaluate the content and make conclusions. Despite the tone in the HN comments, this actually might suggest that the deaths attributed to the vaccine side effect might be significantly higher than the reality but it would take a research to say of this is the case.
I am worried how the discussion around the vaccine has turned political and how there are a lot of strong opinions around it. I worry it might affect funding and also "politically taint" people who publish research about it.
Fair enough but this doesn't mean that the research is finished, just the reporting on it is getting harder. People who actually work with these things instead of pushing their agenda are not really influenced by the politics because what they find is not political. They will not find out that bug Pharma was lying, they will find out how many people actually had myocarditis under what conditions for example.
Fair enough, but everyone was compelled to get the vaccine (regardless of age or risk factors). Given that, the vaccine makers and proponents leave themselves open to such criticisms that would not be valid if the vaccine was not compelled on my 7 year old.
He is acting like it's support of anti-vaxxer claims. And it is why these articles get shared. Because they contain a very slight, practically negligible affirmation of the smallest portion of their claims. And that, in their eyes, is enough to proclaim victory.
If I'm going to read anti vaxxer content I need to be paid, I'm so done finding misrepresentations and statistical hackery in propaganda articles. They cherry pick data, resort in fallacies and all kinds of trickery. They give you a shocking graph where you can see that young people are dying en masse only to find out that this graph is achieved through visual or statistical BS. Hours spend to dig out lies, completely avoidable by avoiding that content.
I'm a little confused here. I'm not trying to convince you of the anti-vaxxer side.
You said:
> "I don't know why the HN comments are acting as if this is some kind of research supporting the anti vaxxer claims."
To which I posted a link of a guy who is acting as if this is some kind of research supporting the anti-vaxxer claims. The comments were trying to head off the exact thing that happened. Because those users know the pattern. They know why this was posted. It was posted specifically as "vindication" for anti-vaxxers. Those comments to point out that this study does not in any way vindicate anti-vaxxers are needed and the people who made them were right to make those comments.
All good then, I just didn't want you to think I was advocating for the anti-vaxxer position. So if that wasn't your intention, apologies to you as well.
And I understand your reluctance. After the nth time, the eyes sort of glaze over as you get slapped with the same bad faith arguments supported by bad logic and supported by abused statistics.
It's not one comment. The guy has a string of them across multiple threads.
And you are going to critique me for "inferring a lot" while ignoring his comment is not only sprinkled with evidence he's a conclusion looking for justification ("lethal jab-associated myocarditis"), but is nothing but inference itself.
This has bugged me since the beginning of this mess. It ought to be possible to say "Hey this looks kind of funny, could the vaccines be having weird effects in this .0000001% of the population?" without daggers coming out all around.
It seems perfectly reasonable to me that "The SARS-Cov-2 vaccines occasionally cause health problems" and "Almost everyone should get vaccinated/boosted" are both entirely true statements.
The issue is that there were coercive government mandates.
"Almost everyone should get vaccinated" does not mean the government should coerce everyone into making the correct medical decision by barring them from employment or access to private establishments.
Absent a very compelling reason, people should be free to go against medical advice. People have the right to do whatever they want with their bodies. People have the right to make the wrong choice.
In this case, the reason given for overriding that freedom was a highly specious argument that the unvaccinated were putting other people at significant risk. That argument did not pass the smell test from the very beginning.
> ...does not mean the government should coerce everyone...
Here you're presuming that the government's role in a pandemic is to wring their hands and issue PSA's. That might be what some folks want them to do these days, but when the legal foundations of public health policy were laid the government was expected to do quite a bit more.
> People have the right to do whatever they want with their bodies.
This might be your opinion, but the majority of your fellow citizens disagree with you. Try asking them about drug use, abortion, suicide, and other "purely personal" matters.
> People have the right to make the wrong choice.
Many wrong choices come with severe state-imposed consequences. We in the US long ago delegated to our elected representatives the authority to force some choices onto individuals, including in a health emergency. We are of course vigorously debating whether they used that authority wisely this time, but it was theirs to use.
> The unvaccinated were filling up the hospitals which was putting other people at risk.
> Your right to gamble with your health ends when you expect to be able to get treatment if the gamble comes out badly.
My right to choose my own treatment outweighs any right you have to feel safer. That includes you feeling safe that the local hospital system will not be at capacity if you have to be admitted.
It’s no different than having a bunch of chain smokers, alcoholics, or morbidly obese people clogging the medical system. People have the right to make potentially destructive choices that are not directly harmful to those around them.
> It’s no different than having a bunch of chain smokers, alcoholics, or morbidly obese people clogging the medical system.
These aren't comparable. Obesity or alcoholism aren't communicable and don't lead to outbreaks. If they did, we'd be having similar discussions as to Covid.
> My right to choose my own treatment outweighs any right you have to feel safer.
No problem. Please sign this document stating that you will not seek treatment for Covid and that hospitals can legally refuse to treat you if you contract Covid.
But, see, that didn't happen. Instead what we wind up with are anti-vaxxers begging for the vaccine after they have been put on ECMO. Yeah, unfortunately it's too late at that point.
And even worse you are now soaking up a hospital bed for 4+ months that should have gone to someone who wasn't stupid.
And even worse that that is the dying person's family giving grief to the hospital staff because someone anti-vax dying of Covid doesn't fit their reality narrative. I could at least have some sympathy for the uneducated following foolish leaders. I have NEGATIVE sympathy for those who then abuse people trying to help them when the consequences come home to roost.
When I can see tears of relief in the eyes of a nurse simply by saying "Don't worry. I'm pro-vax." we have let the idiots have too much leeway.
> No problem. Please sign this document stating that you will not seek treatment for Covid and that hospitals can legally refuse to treat you if you contract Covid.
Why? Do you expect someone who doesn’t get a measles vaccine to sign a waiver refusing treatment if they get I’ll? Do you expect someone who refuses to wear a condom to refuse treatment if they contract an STD?
> Do you expect someone who doesn’t get a measles vaccine to sign a waiver refusing treatment if they get I’ll?
Perhaps? The advantage that we have with measles is that the vaccine can reach "herd immunity" and the measles vaccine is extremely effective. If enough people started dropping the measles vaccine because "Muh Choices!" that we fell below that and it started clogging the hospitals, yeah, maybe. The enclaves that refuse the measles vaccine find out about every 5-10 years why that's a bad idea.
If contracting a bad case of Covid 19 is enough to get anti-vax people to change their beliefs, perhaps that's pretty good evidence that maybe they haven't thought out the consequences of their position very well, after all.
As the kids say: "Fuck around. Find out." Or, as the olds say: "Play stupid games; win stupid prizes."
> The unvaccinated were filling up the hospitals which was putting other people at risk.
Except that wasn't happening, and so much not happening that hospitals were reducing capacity. The emergency capacity built in early 2020 was dismantled after only a month or so and never brought back.
You can find individual hospitals reaching capacity all the time every year forever, but it was never the problem the news made it out to be. Current headlines include gasp hospitals at 80% capacity! ...Except that's normal. The more empty beds they have, the more money they lose - they try to run at around 80-90% full.
Um, obesity is an individual issue (at least at the current levels of hospital load associated with it) so your insurance and bills go up. Unprotected sex has two people involved and can be assault (if not agreed to) and if done by someone who knows they are HIV positive and infects another who dies... manslaughter.
So you filling up ICUs where there's no room for people who bothered to help their fellow citizens with heart attacks, car crashes, or cancer treatment is transmission? That is a different definition of transmission than I am aware of.
Can you please provide a dictionary or other reference?
In case you were wondering when ICUs were full of respiratory diseases, that would be last week.
Wow, what a cherry picked choice, too bad it's still awful and even an overly generous comparison makes that apparent.
There are 23k ICU beds in the US.
The population of the US is 330M.
The hospitalization rate for COVID was ~120/100k in 30 year olds.
Average stay in ICU for COVID was 2-5 weeks.
So if the entire US was made up of unvaxed 30 year olds and 5% of them caught COVID every 2-5 weeks they would require ~3300x120x5%=20k ICU beds for at least an entire year! And since ICUs are normally about 30-50% full with other catastrophic medical events, that means someone else has to die for a self-important exercise of freedumb.
Normally, 30 year olds are healthy and don't present so highly in the hospitals or ICUs so on a percentage basis it's even worse (normal ~2%/decade vs ~20%/decade for 80yrs old). God forbid you're in rural America or your skin color is dark so you don't have access to the beds available in the cities. If you can't be polite to others, you shouldn't expect them to be polite to you.
> The hospitalization rate for COVID was ~120/100k in 30 year olds.
So I think that roughly answers the question, you might expect something like .12 people to be hospitalized (does that include ICU? Do these people have prior exposures? Comorbidities?).
I just ask because I think not everyone is aware yet that covid was (and is) a disease with a wide range of outcomes. I think the number you cited would surprise quite a few people. Many seem to think it was basically like playing russian roulette no matter your situation, and would have guessed a double digit number.
I'm not making any kind of claim that people shouldn't get vaccinated. Just trying to show that some individuals deciding not to get vaccinated isn't exactly as murderous as some might think.
I apologize if this didn't seem like a polite question. Thank you for indulging me.
Sorry, just have immuno-compromised family who are still home bound and couldn't get medical care for more than a year.
I think the other thing that people forget is that covid immune response can give you the same myocarditis (along with clots and heart attacks) as vaccines for much the same reasons, but at higher rates. The fact that the stabilized (Novavax, Pfizer, Moderna) vaccines have 10x lower rates of myocarditis than unmodified spike RNA (ChadOx, Sputnik) indicates that reducing the immune surface variation lowers risk.
As even that top article points out we'd expect the rate of unvaccinated people to approach the base rate which is 76% of the population having received one dose. And since old people are at more risk and are more vaccinated, we'd expect it to reach even higher eventually. But that happens because eventually the unvaccinated do all pick up natural immunity and the effect we're measuring is that the excess load caused by the unvaccinated is declining. We could have gotten to this point much quicker by having 100% vaccination rates (and 100% of the people still being admitted with COVID would then be vaccinated) but with an order of magnitude less load on the hospital system.
The top article you cite has all this information in it, and even mentions the base rate fallacy. It is criticizing the framing of the pandemic as a "pandemic of the unvaccinated" and trying to focus attention on the elderly, but that is orthogonal to the question of if the unvaccinated are disproportionately clogging up the hospital system. Both statistics are true. Everyone should still get vaccinated to reduce the load on the hospital system (although this concern is now fading as antivaxxers actually do pick up immunity the hard way). We should also focus on the elderly more.
As a simple example: if a population begins entirely susceptible and there's a vaccine from day 1 which is available and reduces the risks of hospitalization by 9x and 90% of the people get the vaccine, then the rates of hospitalization will be split 50/50 between the vaccinated and unvaccinated. Vaccinating the rest of the population would increase vaccination rates by 10% but would decrease overall hospitalization rates by 44%.
> the government should coerce everyone into making the correct medical decision by barring them from employment or access to private establishments.
But... the government has been doing that for decades and decades, since the very invention of the vaccine! Why is that "The Issue" when there's suddenly a pandemic and it's important, vs. when you needed to show your vaccination records to join the military or go to school in the 90's or whatever?
You see that the concern you're showing seems, to those of us on the other side, maybe a little insincere?
You see no philosophical difference between the government mandating vaccination records for schools and public institutions like the military vs. them mandating vaccination records for private establishments such as gyms, irrespective of the wishes of the owners of those establishments?
Should the government have the right to mandate vaccination records for entry to a private home, irrespective of the wishes of the homeowner?
Pandemics are not a private issue. It's similar to a war. It can kill a significant percent of the population and it requires collective action to stop it.
The government has the right (and I'd argue, the duty) to quarantine people with diseases that are both contagious and dangerous if that's the best way to keep them from harming others. More details here: https://www.cdc.gov/quarantine/aboutlawsregulationsquarantin...
Your theory is that the best way to prevent AIDS deaths is quarantining people? That seems extreme.
Regardless, it's not one of the diseases listed on the linked page, and it's very different in nature than the ones there, so that sounds like a red herring to me.
You were the only one here suggesting people with HIV were relevant to quarantining. So since neither I nor the CDC thought that was a good idea, then either you did or it was a straw man.
You don't get to dismiss an argument by just declaring that it "didn't pass the smell test." That guidance was exactly in line with every counter-pathogen campaign since, Idk, before germ theory?
The worst part is that we have already comprehensively litigated all of this. The spanish flu had people protesting being forced to wear masks and other societal health measures and the Supreme court affirmed the US's right to mandate those kind of large scale health things.
The mask push then was because, for a while (and despite evidence of infectious agent passing through too-small-for-a-bacterium filters) they believed influenza was being caused by a bacterium, not a virus. Even then, they knew that the masks available would not stop airborne viruses. And masking didn't work then either (areas with enforced masking fared no better than areas where masking was optional). You're welcome to dig into accounts of the pandemic and medical journal articles written during and in the immediate aftermath of the influenza pandemic and confirm this for yourself.
Likewise, the initial (honest) advice not to bother with masks for covid was based on the fact that covid, like other coronaviruses and influenza, is aerosol-borne and aerosol particles pass through surgical mask material easily (so wearing a 2nd tight-fitting mask over a surgical mask to get a better fit doesn't matter).
The u-turn on masks for covid wasn't based on science. The justification later given was that the earlier, correct advice not to bother with masks was a noble lie to conserve supplies of masks for healthcare workers. At the time, the reversal was publicly predicated on hand-wavey (and false) claims that covid might be droplet-spread (droplets are larger than aerosol particles and droplet emissions could conceivably be greatly reduced by well-fitted surgical masks with no gaps).
The initial advice on masks was that we don’t know that they help. This is a truthful and different claim than the claim that we do know they don’t help.
The only record you’ll find of a public health official saying we DO know they DON’T help is USSG Jerome Adams.
It’s weird that you’re writing this implying that we now know masks don’t work. That’s not true. We DO know that SOME masks work, others work hardly at all or none at all.
Yes, the binary thinking unfortunately continues. Masks were/are/will never be 0% or 100% effective. Reducing the number of viruses transmitted at once could mean the difference between life and death for covid though.
Has this kind of vaccine mandate (for everyday life, not for travel) ever been imposed before? I remember the possibility of denying public services (e.g. schooling) to children who weren't vaccinated against measles being discussed but being extremely controversial, and that was for a vaccine that was far more reliable and well-tested.
> It ought to be possible to say "Hey this looks kind of funny, could the vaccines be having weird effects in this .0000001% of the population?" without daggers coming out all around.
That's one in a billion. No, it's not possible to reason about a weird effect affecting less than one person in all of EU + US combined.
But we do actually know what happens when there is a legit safety concern with the vaccines affecting a slice of the population, since it has happened. The AZ vaccine turned out to have rare (but not one in a billion rare), serious and even lethal, complications for young women. The public health authorities picked up on this within a month, and acted to stop the use of that vaccine first for that at-risk group and later for everyone.
But the same people who believe that evolution and climate change are hoaxes are also convinced that COVID is a hoax. (The disease is a hoax, the vaccine is a hoax, the hoax disease that doesn't need to be cured by the hoax vaccine is an attack by China -- and the coverup is a hoax.)
And those people are ~40% of the US population, with an outsized thumb on the scale of elections due to accidents of geography and history. So instead of talking cogently about tradeoffs, we're barely fending off turning conspiracy theories into policy. And by "barely" I mean "succeeding slightly more often than we fail".
Yeah, we ought to be able to discuss things cogently. That ship sailed a long time ago.
> I am vaccinated but I am upvoting this post because I believe that it is important to investigate these cases to determine how to improve future vaccines.
The fact that people feel the need to say that for any criticism of an intervention says that we have long left the realm of science and entered the realm of religion.
Every intervention has benefits and harms.
Not talking about harms makes it impossible to assess the cost-benefit tradeoffs of the intervention.
I agree with you, there’s a weirdly political zealotry when it comes to such things.
I took the Sinopharm vac as I felt hesitant to take what I considered to be brand new tech in the MRNA vaccines (I ended up taking the MRNA one as well but that was for travel reasons where I live). And people online acted like I was a conspiracy theorist, for preferring the tried and tested tech of the traditional vaccine.
I keep hearing vaccination being promoted, but the last major study I saw showed no statistically significant difference in natural immunity + vaccination versus simple natural immunity. This also seems to be a topic treated as a fringe conspiracy theory instead of an extremely serious health issue worthy of a large amount of resources dedicated to giving us an answer. One certainly could be forgiven for thinking the vaccine has become a larger political issue than health issue for both sides.
> As long as vaccine side effects cause less deaths and less harm than the virus, vaccination is still the way to go.
No.
This is the wrong criteria to judge by. Right now it takes ~30,000 injections to prevent one hospitalization from COVID, according to recent studies.
So the real criteria is, if there are severe side effects in more than 1/30k they should be pulled.
In Pfizer's own RCT more people died in the vaccinated cohort. They had ~4x the amount of cardiac arrest. There was no proven effect on all-cause mortality from the start. Anyone paying attention and not blindly listening to politicians and the sycophantic media knew this long ago.
Wife got shot. Few days later her arm swelled up. 2 years later it still is. Her and I had already had Covid from before the vaccine. Absolutely refused to get it because of that. She now regrets it. She still gets Covid with every outbreak anyway. So doesn’t seem to have helped.
I know a couple of kids that got it and have clots in their brains now. Less sure on timeline on these. But I’ve not seen this before.
Sure it could all be coincidence.
then there’s all the assholes who decided that get the vaccine or become unemployed.
Another thing that hasn't gotten enough research is the effectiveness of the latest booster for someone who was vaccinated earlier and got omicron (this is a pretty big cohort). It's genuinely hard to make a recommendation one way or another on it because it's not clear how effective it is after four prior exposure events, and it has to be weighed against the risk of side effects like this.
Same. The impact rate of myocarditis might be extremely small, but if it's caused by the vaccine, it should be investigated, while at the same time, people should get vaccinated.
Luckily, the scientific community understands that.
Unluckily, the non-scientific community doesn't on both ends.
The supporters of the vaccine think you're attacking the vaccine. The detractors think you're suddenly supporting them.
No. EVERYONE should be vaccinated. The vaccine has been given to billions, it is exceedingly safe. Can we do better? Yes. Is it marginal? Also yes, but I don't wish miocarditis on anyone.
I agree it is good we keep funding studies to try to better understand and predict the effects of the vaccines. What would it mean to feel like we have a good understanding though? How would we quantify "god"? We have observed that the side-effects have minimal deviation from the normal variations observed in the population for those effects. And we also know it is highly dependent on individual characteristics as to who exhibits the worst side-effects or best antibody response.
> What would it mean to feel like we have a good understanding though? How would we quantify "god"?
That is a hard question and honestly I don't have the knowledge to answer it.
> We have observed that the side-effects have minimal deviation from the normal variations observed in the population for those effects. And we also know it is highly dependent on individual characteristics as to who exhibits the worst side-effects or best antibody response.
Yeah, I get that the vaccine can cause side effects for a very small minority of the population. I think what I want is for vaccine side-effects to be treated more like plane crashes. I get that bad things happen, but if it isn't cost-prohibitive, I would like to know why these things happened, even if they happen extremely rarely.
I'm pretty sure that's how medicine works. Obviously, if I knew the vaccine would kill me, I would not take it. But it's the same deal with literally any medication.
When I was prescribed Accutane for my acne, I was told that it could cause kidney damage. If I knew it would cause kidney damage to me would I have taken it? Of course not. But I hedged my bets and gambled that it wouldn't.
As far as the suppression of information goes, obviously that is totally unacceptable. That's also partially why I upvoted this post right?
Has there been any plan to compensate victims of the vaccines? either deaths or heart inflammation or other side effects?
Any plan to approve and understand vaccine's effects should also come with proper system to compensate and acknowledge the risks.. But I feel that this has been avoided from the start to remove any liability.
Yes, it’s never either or. For one good example of the complexity, see this video [1] where Paul Offit notes the problems with the current bivalve that vaccines.
The association between heart problems and mRNA vaccines is a settled matter - outside social media at least.
The Paul Ehrlich institute which is monitoring vaccine side-effects has a nice detailed report on vaccine safety with details on heart problems and all sorts of other things.
Most affected are men and male teens between 12-17 and Moderna’s causing more problems than Biontech. This was the main reason why the German vaccination committee recommended that men under 30 get Biontech.
I missed “settled matter” in the scientific method handbook. The reality is that this experiment is still unfolding and will continue for the rest of my life. It will take decades of research and observations to have real answers.
> As long as vaccine side effects cause less deaths and less harm than the virus, vaccination is still the way to go.
Assuming the vaccine prevents or lessens the effects of infection, this is logical. A common belief is that the vaccine is virtually useless. If this belief is true or close to true, then taking the vaccine would result in an increase in risk.
> Standardized autopsies were performed on 25 persons who had died unexpectedly and within 20 days after anti-SARS-CoV-2 vaccination. In four patients who received a mRNA vaccination, we identified acute (epi-)myocarditis without detection of another significant disease or health constellation that may have caused an unexpected death.
Myocarditis was found in 4 out of 25 people who had received the vaccine and died within 25 days of it, and none had showed any sign of related disease.
What are the odds of any 4 out 25 people in the age range of the group with no record of any related illness having acute myocarditis?
It is so typical of HN that your vapid comment should rise to the top.
> Currently, I still believe that people should vaccinate, even if vaccines cause mortality/harm in some cases. As long as vaccine side effects cause less deaths and less harm than the virus, vaccination is still the way to go.
Where is the evidence of this, given that many governments have withdrawn the vaccines or even banned for them for young people, a category you probably fall into?
> What are the odds of any 4 out 25 people with no record of any related illness dying of myocarditis.
Note that I'm not saying vaccines do not cause myocarditis, I'm saying that even if vaccines may cause myocarditis but cause fewer myocarditis cases than COVID deaths, then it is still worth vaccinating.
> Where is the evidence of this, given that many governments have withdrawn the vaccines or even banned for them for young people, a category you probably fall into?
Hence my next sentence right?
> My position depends on us having a good understanding of the vaccine's effects however, and right now I feel like we don't.
That said, although I didn't mention it in my comment, my current understanding of the statistics does make me believe that the vaccine causes less cases of myocarditis than COVID deaths.
Schauer J. et al: Persistent Cardiac Magnetic Resonance Imaging Finfings
in a Cohort of Adolescents with Post-Coronavirus Disease 2019 mRNA
Vaccine Myopericarditis, The Journal of Pediatrics, March 25, 2022
https://www.jpeds.com/article/S0022-3476(22)00282-7/fulltext
Chua G.T.et al: Epidemiology of Acute Myocarditis/Pericarditis in Hong
Kong Adolescents Following Comirnaty Vaccination, Clin Infect Dis 2022,
Sep 10. 75(4):673-681
https://pubmed.ncbi.nlm.nih.gov/34849657/
Massari M. et al: Postmarketing active surveillance of myokarditis and
pericarditis following vaccination with COVID-19 mRNA vaccines in
persons aged 12 to 39 years in Italy: A multi-database, self-controlled
case series study, Plos Medicine, July 2022
https://pubmed.ncbi.nlm.nih.gov/34849657/
In Czechia, quite respected medium blame inflation and high prices for energy the reason of higher heart failures. No words about possibly side effect of vaccines.
But it's not surprise when gonverment bought 20 milion doses for 10 milion nation in spring 2022 for 7,5 bilion CZK when most are done with vaccination for covid. In 2023 they plan buy even more for another 5,5 bilion CZK. Thats how corrupted our gonverment is.
I had a bad reaction to an mRNA vaccine that I’m still dealing with, and feel exactly the same as you do. This technology is too important to politicise. We need to look at it scientifically, make it better, and continue to deploy it in situations where the risk profile makes sense.
The last paragraph in the article literally indicates there is no causal relationship or proof of any direct link between the vaccination and myocarditis.
> "Finally, we cannot provide a definitive functional proof or a direct causal link between vaccination and myocarditis."
It's also important to note that although they looked at 35 autopsies for people who died in the period after vaccination, only 4 of them had signs of myocarditis. 10 of them had very clearly unrelated causes of death (e.g. pre-existing conditions, easily identifiable external causes). I don't think people realize just how frequent death, including unexplained death, can be when you're looking at population-level sample sizes:
> In four patients who received a mRNA vaccination, we identified acute (epi-)myocarditis without detection of another significant disease or health constellation that may have caused an unexpected death.
They found some interesting clues that suggest it might be related to accidental intravascular injection:
> Interestingly, we recorded inflammatory foci predominantly in the right heart, which may suggest a gradual blood-stream derived dilution effect and based on this finding it is at least tempting to speculate that inadvertent intravascular vaccine injection may be contributive.
> In general, a causal link between myocarditis and anti-SARS-CoV-2 vaccination is supported by several considerations: (A) a close temporal relation to vaccination; all cases were found dead within one week after vaccination, (B) absence of any other significant pre-existing heart disease, especially ischaemic heart disease or cardiomyopathy, (C) negative testing for potential myocarditis-causing infectious agents, (D) presence of a peculiar CD4 predominant T-cell infiltrate, suggesting an immune mediated mechanism
> In general, a causal link between myocarditis and anti-SARS-CoV-2 vaccination is supported by several considerations: (A) a close temporal relation to vaccination; all cases were found dead within one week after vaccination...
> Standardized autopsies were performed on 25 persons who had died unexpectedly and within 20 days after anti-SARS-CoV-2 vaccination.
This is a weird way of demonstrating a link. They picked them specifically for that, it can't be evidence of something. If they selected 25 people who died of myocarditis regardless of vaccination status or recency, and all 25 turned out to have been recently vaccinated, that would be scary data.
>This is a weird way of demonstrating a link. They picked them specifically for that, it can't be evidence of something. If they selected 25 people who died of myocarditis regardless of vaccination status or recency, and all 25 turned out to have been recently vaccinated, that would be scary data.
It's perfectly valid as an idea, although a lot of statistical work would need to be done to show that it wasn't just happenstance and/or rule out other causes. But a link, sure.
Consider a depoliticized example: you do 30 autopsies on people who had recently been to a particular location, let's say a certain grocery store in town. Enough people go to this grocery store that it's not uncommon for way more than 30 recent visitors to be dead unexpectedly by random chance. Further, let's say in the general population, a tiny fraction of people die of a certain food-borne illness. You have a pretty good guess what that fraction is.
You do these autopsies and you find that 5 of the people died of this food-borne illness. Much higher than the proportion in the population. Now, you have a lot of additional work to do before you prove that something at the store is causing high rates of the illness: check on comorbidities, other correlated factors, plenty still to be done. But, have you established a potential link? Sure. And you picked them specifically because they died after going to this store.
Also, your idea can work too, also with appropriate statistical work, experimental design, all that. Yours is perhaps a bit better suited to answering a question like: of those who die of myocarditis, what proportion have been recently vaccinated? While a proper study the way the authors did is more like: of those who are recently vaccinated and die unexpectedly, what proportion have myocarditis? Both are valid questions and both certainly get at aspects of the link between the vaccine and myocarditis.
> Consider a depoliticized example: you do 30 autopsies on people who had recently been to a particular location, let's say a certain grocery store in town. Enough people go to this grocery store that it's not uncommon for way more than 30 recent visitors to be dead unexpectedly by random chance. Further, let's say in the general population, a tiny fraction of people die of a certain food-borne illness. You have a pretty good guess what that fraction is.
It's not just "pick 30 recently dead who went to the store", though.
You've picked 30 people who died after eating at the grocery store's salad bar, and used that as evidence that the salad bar is dangerous, without checking how many skipped the salad bar and died anyways.
>You've picked 30 people who died after eating at the grocery store's salad bar, and used that as evidence that the salad bar is dangerous, without checking how many skipped the salad bar and died anyways.
The answer to this question would also be socially and politically relevant and warrant its own study. But that doesn't make the author's study unsound or unable to serve as evidence, like you said.
From published articles in the JAMA; vaccination related myocarditis in young men has much lower mortality and morbidity than from other causes. So were really talking about two different things here.
The second is rates of myocarditis after vaccination and the population base rate aren't the same thing either. The base rate one assumes includes cases triggered by something. So the base rate incorporates the rate of triggering events. So these rates are also not the same thing.
The causal link (direct or otherwise, does it really matter to most people) between vaccination and myocarditis has been established elsewhere and acknowledged by the CDC.
But in the intro:
>> Thus, myocarditis can be a potentially lethal complication following mRNA-based anti-SARS-CoV-2 vaccination.
I would assume that means there is something going on.
To your point, medical researchers are IMHO kind of bad at accepting reality if they don't have a complete understanding. So if data show death by specific cause after vaccination, they will reject that conclusion if there is no proven mechanism for it. Rather than critique the study, they simply demand more information than anyone has.
TL;DR: The study is fraudulent as it didn't normalize for distance or time driving, which has a extremely strong correlation to traffic fatalities. What the study actually found is that the unvaccinated drive more, and reporting it the other way was intentional fraud.
That's not what it says. I will give you an example. Before the 1980s or so when the first serious studies on second-hand smoke exposure were conducted, anybody could have also written that "we cannot provide a definitive causal link between second-hand smoke and lung cancer." Today, it is common sense.
No, it's not common sense. It's science, proven over decades and presented to people in an understandable way so that were willing to adopt it as a belief they hold.
Common sense nonsense:
You can fall off the edge of the world
You should put ice on burns
We only use 10% of our brain
"Interestingly, we recorded inflammatory foci predominantly in the right heart, which may suggest a gradual blood-stream derived dilution effect and based on this finding it is at least tempting to speculate that inadvertent intravascular vaccine injection may be contributive."
Does this indicate that the authors believe aspirating the vaccine during administration would reduce the risk of myocarditis? I don't have a biological background so I would be interested in hearing someone else's take on this but that sentence seems to indicate that the authors think ensuring correct administration would lower the risk of post-vaccine complications (which from what I've seen, remains low but non-zero). If that's the case, then perhaps the issue isn't as much with the vaccine itself as how it's being administered.
Yes. Complication from jab administration is something that has been widely discussed (not widely reported though). The clinical trials were supposed to show that the jab (and therefore the mRNA, and the resultant spike protein generated, which is known to be toxic) stayed in the muscle local to the injection site.
What is widely speculated is that on some not-insubstantial portion of injections, the jab makes it into the bloodstream. This would explain why we see spike protein collecting in the heart, reproductive organs and other parts of the body.
And because of how the jab works - inducing spike protein genesis as well as an immune response - when the immune system finds spike protein on the cells that are creating it (supposed to be just your arm muscle but ends up being your heart and other things), it starts attacking those cells. Which leads to inflammation, blood clots, etc.
A nurse friend of mine raised this as a concern. The protocol for intramuscular injections used to be (and in some places still is) to draw the plunger back a bit first to verify that you're in muscle, and haven't hit a small vein. If you pull blood, you find new spot.
In practice this doesn't happen for covid vaccines, and her personal hypothesis was that many of the adverse reactions (myocarditis, or just being hit hard) were due to the vaccine partially being administered into a vein.
> The clinical trials were supposed to show that the jab (and therefore the mRNA, and the resultant spike protein generated, which is known to be toxic) stayed in the muscle local to the injection site.
They didn't. The data Pfizer released to the Japanese government showed that the lipid nanoparticle could be found all over the bodies of the test rats in hours. It's a small proportion of the overall shot, but the data only goes to 48 hours and in most areas (particularly the ovaries, which is what people kept calling out from this) it was still increasing.
This is extremely fascinating to me as a layperson. Can you explain how this effect would be unique to mRNA? Like, could you get a flu shot and end up with some of the inactivated flu virus spreading around the body and sticking to other organs? Or is the spike protein collecting in other organs solely because the mRNA is telling those cells to produce it, whereas with a typical vaccine the dead virus could get into the bloodstream but it would simply float around the body without piling up anywhere til it's taken out by the immune system?
The difference between the covid jab and the flu vax has to do with the combination of a) mRNA turns your body into a "factory" to pump out a somewhat-unknowable and individually variable quantity of spike protein, and b) the spike protein "sticks to organs" as you put it (or more generally, is harmful), which is not something that e.g. a deactivated virion does
Or, maybe that leads to more vasculature and more chance of hitting a vein? It's interesting that it was more prevalent in young men than other demographics.
For a long time this theory always made the most sense to me, and frankly I assume I must just be missing something since it’s so obviously criminal if there was a chance this was true that it wasn’t blasted from the rooftops from the CDC (for the public to help correct it when they got their vaccine.)
>>The reported incidence of (epi-)myocarditis after vaccination is low and the risks of hospitalization and death associated with COVID-19 are stated to be greater than the recorded risk associated with COVID-19 vaccination [29].
the more interesting unaddressed question is, for whom? i am a young-ish healthy person, i have basically no risk of ending up in the hospital for covid. what is the risk tradeoff for people similar to me, rather than an abstraction of the entire population? what is the risk tradeoff for a young child, who effectively has zero risk of serious covid?
> what is the risk tradeoff for a young child, who effectively has zero risk of serious covid?
This is only true if you consider death the only "serious" outcome. Around 25% of children and adolescents who get COVID-19 will get "long COVID", with long-term effects we've just begun to understand. Plenty of "young-ish healthy people" have suffered debilitating effects.
A 14℅ reduction in something that happens to 5%+ of people measurably and probably lowers your developmental outcome even if it is bellow the threshold of clear measure (a weaker school year that you never quite catch up from could just be random after all.)
That's a much bigger deal than whether you have 12 in a million or 24 in a million chance of something that has a 5% chance of being fatal.
Giving a population lead poisoning didn't kill any of them outright but cognitive problems in the lead generation is correlated to our higher homicide rates and many of the poorer outcomes in our generation and echo's of its affects in society.
I find it interesting that the wider anti-vax demographics overlap heavily with the safety/helicopter parenting that focuses on some extremely unlikely demise as a reason to limit the next generation in ways that will have much higher rates of earlier deaths and reduced lifestyles when considering their overall lifespan.
You sound like somebody that likes to crunch numbers, but doesn’t understand how most parents decide on these things. Or if you happen to have children, you’re unusually clinical about their health…
Anyway, the children’s vaccine was authorized in the EU on the 19th of October 2022, after all Omicron strains were making rounds through the population.
In Germany at first one dose was recommended for 12-17 then one plus booster. Kids younger than 12 may be vaccinated on a case by case basis if there’s risk factors or the parent explicitly wants it. This means that the risk of Long Covid in this age range is not a “bigger deal” than the benefits and risk from the vaccine.
According to the RKI, there were 1500 vaccinated in the age range 0-4. And between <10% and 30% in the range 5-12 depending on state.
In conclusion, your dogmatic approach is not supported by the competent health organizations. Neither is it supported by parents.
> doesn't understand how most parents decide on these things
> your dogmatic approach is not ... supported by parents
Your dogma here is that you assume all parents take the zero-sum "ok for thine but not for mine" approach. Personally I know plenty of parents who were eager to vaccinate their kids against COVID. But I'm not taking my personal outlook as some kind of fact about all parents.
Instead I will note that in the history of vaccine mandates there has always been opposition from a _minority_ of parents, doctors what have you in the context of broad societal support, even though vaccines have always had some amount of risk that similarly to COVID were vastly outweighed by the societal benefit and the risks of the disease itself.
You naughtily cut my quote and removed “supported by the competent health organizations”. I added that back for you.
Allow me to expand on that: the parents which didn’t vaccinate their children (<12) are the ones who are in agreement with “the science” and they are the majority. I’ve provided numbers for Germany from the appropriate health organizations.
The parents that vaccinated their healthy kids are the ones that decided based on feelings or were influenced and manipulated by vaccine activists.
The risk to society must be handled by the society, not kids. Adults are welcome to wear masks or get the vaccine themselves. Or they can choose to die free, choking on their own mucus like a boss.
The risk of the disease is obviously not that great to kids (<12) according to the vaccine commission. Almost looks like adults are trying to force kids into a treatment so that said adults benefit.
i believe i have found the source[0] for your claim -- this seems a bit overplayed as 'long covid' when the definition is given as any persistent symptom, including congestion and emotional state(?)
Essentially all children and adolescents will get Covid if they somehow haven't had it already. Something like a quarter of the population being physically disabled to even a mild degree is an extraordinary claim requiring evidence in kind.
A survey essentially asking people "do you have long covid?" isn't extraordinary evidence. Could be a simple case of psychogenesis[0] like has been common during any mass illness event historically. The demographic info in your link seems to indicate that is a possibility. With 25 percent of the population apparently having this disease it's not a hard one to study experimentally.
That's not even the complete question though -- because by all accounts, Covid actually results in a higher incidence of myocarditis than the vaccine does.. Given the tenor of the conspiracy theories here, the landscape of questions is too nuanced for HN I guess. Ideally, the vaccine recommendation would weigh:
Incidence and seriousness of myocarditis (ISM) naturally / in absence of covid or vaccine, ISM following vaccine, ISM following Covid, ISM after being vaccinated but later catching Covid, relative risk of death / or the other litany of problems following unvaccinated covid infection, same but with vaccinated covid infection and the increased chances of avoiding infection after being vaccinated.
It's possible that vaccines are leading to more myocarditis, covid is certainly leading to more myocarditis, most cases of myocarditis are undetected and resolve on their own with no health impact at all.. as expected, weird antivaxxers are harping on point 1 to the detriment of anyone actually interested in public health.
statistically, it is extremely unlikely[0] for an otherwise healthy young person to end up in the hospital for covid, much like myocarditis -- i am simply interested in which is more likely for specific population subsets
The numbers are so small that it is hard to say -- several long-term studies are ongoing. All the evidence suggests the risk of Covid is far greater. I'm sure you know this, but covid causes significantly more cases of myocarditis than the vaccine.
During the past 60 days for people 18-49 (the cohort sizes are suspect) COVID cases per 100,000 were as follows:
Not fully vaxxed: 98.0
Fully vaxxed: 70.3
Boosted: 92.8
For 49-64 (again with the cohort sizing) per 100,000 cases are:
Not fully vaxxed: 90.0
Fully vaxxed: 86.7
Boosted: 96.7
Over 65 cases:
Not fully vaxxed: 390.05
Fully vaxxed: 284.2
Boosted: 161.7
So if you're young and healthy if you're boosted, you're hardly getting any protection.
If you're middle aged, it doesn't look like you're getting any protection from getting infected and if you're boosted, you may be increasing your risk.
If you're old and vulnerable, you should absolutely take the vaccine.
The CDC summarizes and caveats the data as follows (note particularly the last point):
- All vaccinated groups had overall lower risk of dying from COVID-19 and testing positive for COVID-19 compared with people who were unvaccinated.
- Based on early surveillance data, people who were vaccinated with an updated (bivalent) booster dose had lower rates of dying from COVID-19 and slightly lower rates of testing positive for COVID-19 compared with people who were vaccinated but had not received an updated booster dose.
- Age-standardized rates of cases and deaths by vaccination status and receipt of the updated (bivalent) booster dose do not account for other factors like the higher prevalence of previous infection among the unvaccinated and un-boosted groups; waning protection related to time since vaccination; and testing practices (such as use of at-home tests), underlying conditions, and prevention behaviors which likely differ by age and vaccination status. Additionally, any data recording errors that misclassify monovalent and updated (bivalent) boosters at the time of vaccine administration would make rates between the two groups appear more similar.
Lumping all people over the age of 12 together doesn't address what I was saying. I used the data I could find that had cohorts by age and vaccination status. I'm trying to dig through your source to see what the numbers look like per age cohort. I'm assuming we are going to find similar numbers in your data as we did in the MN data.
As for 60 days, that seems fair as that's likely to capture the prevalence of the most recent variants and not delta, which we know the vaccine worked well against...
So, looking at your source for the last 60 days, if you're in the 18-49 range your likelihood of getting Covid is about 2x if you're not vaxed and 2.2x if your not boosted.
Getting covid once right after sleeping in same space with all vaccinated. Positive - stayed at home - pretended to be ill. Friend, vaccinated, panicking getting covid after vacc..
Buut..this is Divide and Conquer, don't you see?
"stated" is an interesting choice there, especially when using "recorded" a few words later. It reads as being a bit untrusting of the COVID death numbers.
An article was published in Nature a few days ago saying the actual number of COVID deaths could be around 2.75x higher than officially reported numbers. We might be underestimating deaths by many millions worldwide.
If it was one general noisy correlation, I would agree. But there are multiple spikes that go up and down and match almost precisely with the multiple waves of covid, persisting through many shifts in other factors (like downstream effects of different levels of lockdown) with almost no change in the trends for all other deaths beside it. It's about as close of a correlation as you can ever hope for with real-world data.
Which of them do you propose would cause the American public (and others worldwide; we see excess deaths increased everywhere, whether they required masking or closed schools or did very little to mitigate) to suddenly start dying in significantly higher numbers - again, of any cause - for the last two years - and especially so at the same time large COVID waves are occurring?
> Which of them do you propose would cause the American public (and others worldwide; we see excess deaths increased everywhere, whether they required masking or closed schools or did very little to mitigate) to suddenly start dying in significantly higher numbers - again, of any cause - for the last two years - and especially so at the same time large COVID waves are occurring?
I can give one example, which happened to my dad...
"Sorry, we have to reschedule that surgery to remove the tumor because we're anticipating a covid spike and need the bed availability."
That sort of thing is relatively trivial to tease out of the stats, because in addition to excess deaths we have per-disease statistics as well.
See the chart about 2/3 down on https://www.healthsystemtracker.org/brief/covid-19-continues..., titled "Average daily deaths in the United States, by cause (2020 - Present)". We don't see a massive spike in other causes of death (including cancer, which is a flat line at ~1,600/day throughout), and no one's likely to misidentify a cancer or heart attack death on a death certificate.
There are certainly cases like your dad's, where delayed screenings and treatment had individual impacts, but none of the stats available to us show this explaining a meaningful amount of the 1.3M excess deaths observed.
It's actually a non sequitur because you can still get Covid after getting the vaccine. It's not an either/or at all, and in fact most people who got the vaccine did get Covid.
Why is it so hard to find data showing how often people are dying, no matter the cause, broken down by vaccination status and age? Surely that would help clear things up. Lots of countries publish COVID-19 mortality rates which show benefits for vaccinated but that's really not helpful for understanding overall risk of vaccines. The UK is the only country I could find that publishes this data and unless I'm missing something things look really bad. Table 2 in [1] shows a 2-3x higher mortality rate for vaccinated vs. unvaccinated in almost all groups this year. Perhaps the unvaccinated are healthier on average, maybe, but 2-3x healthier? Yeah, don't think so. What's going on?
That is showing the raw numbers - they aren't adjusted for vaccinated/unvaccinated population sizes. ~53 million people have had at least one shot, and there are around 6 million children under 10 (so not counted in the figures you linked). With a population of about 68 million total, the unvaccinated all causes figures should be about 16% of the ever vaccinated.
The ratio should skew further in older age ranges, as a higher proportion of those were vaccinated.
It also shows mortality rates per 100,000. That's what I was referring to. For example, here are the rates of all-cause mortality for the most last month they released, May 2022, for the 40-49 group:
Lest someone draw the statistically unsound but temping surface level conclusion from this, consider that people with pre-existing conditions and especially severe ones would have more incentive to have three doses. There is self selection on these groups, they are not random samples.
For it to be a reasonable choice to not want to take the vaccine wouldn't you need to balance the risk of death / complications from the vaccine against the risk of death / complications from covid multiplied by the risk of getting covid?
There seems to be a lot of "aha I knew it" whenever any side-effect of the vaccine is found, but aren't the side-effects of covid well established, on average more severe, and much more common?
According to my governments stats, the COVID-19 hospitalization rate for my age + health cohort, when modestly adjusted for their known undercount of cases, is less than 1 in 3000.
Also by their stats, more than 1 in 2000 4-dose mRNA vaccine series have resulted in a serious adverse event reported by a health professional.
Then, factoring in the additional risk of acquiescing bodily autonomy to an opaque bureaucracy — considering what herding behaviors have been blatantly manufactured over the last few years, and the conflicting interests involved.
Don't forget natural/recovered immunity, which people seem to finally be considering again. For a lot of people any vaccination was unnecessary risk for no reward.
What constitutes a 'serious adverse event' in this data? Do you mind linking the source? Having a 1 in 3000 chance of getting so sick you need to be hospitalized seems quite bad.
1 in 9000 doses reportedly results in a SAE, so if you are mandated to take 4 doses, your risk becomes ~0.04% or ~1/2500.
This also does not factor in the risk of "adverse events of special interest", which can be serious or non-serious (though neither seems great for the end user).
And looking at how this page has been updated since the last time I saw it, another red flag is how they separate those out - with a dead link to boot. In my opinion a continuation of efforts that seem intent on obfuscating the ability to make individual risk calculations through this pandemic.
> 1 in 9000 doses reportedly results in a SAE, so if you are mandated to take 4 doses, your risk becomes ~0.04% or ~1/2500.
That sounds like motivated bad assumptions.
Seems highly plausible that those who would get the reaction in the 1/9000 would select out the sensitive individuals so the rate would be less for subsequent shots on the other 8999. It seems very unlikely it will be a constant rate.
Anecdotally, I had the same reaction to all four shots. Mild symptoms the lasting 24 hours. With your comment’s assumption that’s pretty statistically unlikely, statistically it would have been likely that one would have been less or more, since by your comments logic it’s completely random.
I'm looking at your link but I can't find anything about serious events controlled for age group (to make it a fair comparison to your covid hostpitalisation number). Is the data in there somewhere?
Would be nice, but all they volunteer is that the adverse event rate is highest in the 30-50 year olds. Given that, I don’t think it makes a material difference
Inference based on overall adverse events post-vaccination being lowest in elderly recipients, plus the early SAE warnings (myocarditis, etc.) being exclusively towards young adults.
Also more conspiratorially, because I think they would have provided the age-stratified data if it supported their objectives of improving lagging uptake among younger cohorts.
In case they don't answer, I would guess they are referring to VAERS data, and some random guy who once claimed it underreports everything by 40x. This is not logistically plausible (where would you hide 40x more patients than expected arriving at hospitals?), and I have seen some recent studies suggest that the underreporting factor is actually <1x (meaning it is overreported) when doing statistically random sampling. But that does not stop people from repeating the claim ad nauseam.
In Canada, all reports to our Public Health Infobase must be made by a health care professional. I do suspect underreporting, given social and collegial pressure on practitioners to not undermine vaccination efforts, but I accept the given stats linked above at face value for the purposes of my model.
the 40x is possible, and even likely - but that is often twisted to suggest that if there were (for example) 10,000 reported deaths in vaers, then it must mean there were 400,000 actual deaths from the vaccine - yes, there is a lot of under-reporting, and maybe even a 40x factor, but those unreported events are usually of the trivial kind - i.e. 'I had a sore arm after getting the shot' - likely trivial symptoms are under-reported by quite a bit - not plausible that there are 40 deaths for every reported one.
> For it to be a reasonable choice to not want to take the vaccine wouldn't you need to balance the risk of death / complications from the vaccine against the risk of death / complications from covid multiplied by the risk of getting covid?
Reasonable is subjective. I got the covid vaccine and had no concern for side effects. But I, like most people, don't bother getting the flu shot every year and I think that's perfectly reasonable despite me having no qualms about side effects. I simply don't care about the flu. Not getting the flu shot is one less reoccurring chore in my life that I don't have to bother with.
Every person I've asked (here in Sweden) who opted out of COVID-19 vaccination made their decision based on one year of case data covering the two first waves, which to them concluded that statistically they were at no risk based on their age and health status. Despite taking e.g. tetanus boosters, TBC vaccine etc., they are still being referred to as "antivaxxers".
I don't know what stupid assumptions you're making, so I'll fill you in:
The Swedish National Board of Health and Welfare has been producing thorough public statistics over the situation in Sweden ever since the COVID outbreak began. The statistics are accumulated on a weekly basis and cover the number of confirmed infections, number of mild and severe hospitalizations, and the number of deaths. All of it is broken down in age groups as well as grouped according to prior underlying health concerns of the patients.
The statistics accumulated up to the same week the general availability vaccinations began - covering two waves and approx. 14 months of COVID - revealed that for their age group (age 35-45) and with no known underlying health problems, there had been a total of 11 deaths. It's fully understandable that they don't feel threatened by this virus.
Today the accumulated statistics for the same period states this:
Total number of hospitalizations, age group 40-49: 4281
...of which had one or more prior health problems: 65.5%
Total deaths, age group 0-49 (reported as "below 50"): 121
...of which had one or more prior health problems: 85%
Just winging it for healthy adults in age group 40-49: 1050 hospitalizations, fewer than 19 deaths.
> to be a reasonable choice to not want to take the vaccine wouldn't you need to balance the risk of death / complications from the vaccine against the risk of death / complications from covid multiplied by the risk of getting covid
No.
Reasonable people make choices all the time that don't bear out under a cost-risk-benefit analysis like you propose. Those choices are still reasonable, despite perhaps not being strictly rational.
And certainly not as a matter of public policy. The value of individual freedom of choice is inherent unless there's an overwhelming and compelling reason to violate it.
There is far, far greater danger in society forcing issues of bodily autonomy to a vote than there is in someone eating too much sugar.
The comment you replied to didn't mention mandates of any sort. It started with:
> For it to be a reasonable choice to not want to take the vaccine
"Basically everyone should get the vaccine" is a meaningfully different statement from "we should force people to get the vaccine".
Also, whether a person can be reasonable while making unreasonable choices isn't really the point either. The most reasonable option on this particular choice for the overwhelming majority pretty clearly seems to be to get the vaccine. It is similarly disingenuous to move the goal posts from "the most reasonable decision is to get the vaccine" to "you are an unreasonable person to not get the vaccine".
No. Reasonable decisions are literally defined as "what a reasonable person would do." What is disingenuous and dishonest is moving goal posts from "a reasonable choice" to "the most reasonable decision."
It's true that the post didn't mention mandates, but any time a group of people are putting themselves in the position to decide whether a person's individual choice about their own body is "reasonable" or not, you are pretty damn mandate-adjacent.
The choices are acceptable, not reasonable. At least by the strict definition of reasonable -- we seem to be changing that definition similar to the world
"literally."
> The value of individual freedom of choice is inherent unless there's an overwhelming and compelling reason to violate it.
This is a slippery slope easily. People should be given the choice.
And as people we have also the choice to judge people on their choice's results.
Especially if it causes other people to die. Right now we have failed as humanity at least 6,637,512 people and counting.
My question wasn't about public policy or mandates, I'm asking what data an individual is looking at to come to the conclusion that not getting vaccinated is the right choice.
>For it to be a reasonable choice to not want to take the vaccine wouldn't you need to balance the risk of death / complications from the vaccine against the risk of death / complications from covid multiplied by the risk of getting covid?
a huge chunk of the population already got covid during the entire year no vaccine existed and have natural immunity, so that's not really a factor at this point. The risk of getting covid for them is already baked into the calculation because they got it when there was no other option. They can now decide whether the additional risk of the vaccine is worth it
you can't even make the case for mandates based on "stopping the spread" anymore because the vaccines failed at that as well, so it's no longer a public health issue and becomes a personal health decision. Or at least it should be
> a huge chunk of the population already got covid during the entire year no vaccine existed and have natural immunity, so that's not really a factor at this point.
The new variants are effective at evading immunity from earlier variants so, no, that's not moot. Even without evasion you'd still need to consider how quickly immunity wanes, too. The vaccines are holding up well for avoiding hospitalization but you're still looking at multiple per year given how much COVID has been mutating.
I've got two Pfizer shots but I know many vaccine skeptics who refused to take the shots and they aren't skeptics because of the risk/reward ratio of the vaccine vs covid. They're skeptics because the politicians and the media have repeated a great many different lies during this entire fiasco.
For a start if people were allowed to discuss the lab leak hypothesis without being called moon-landing deniers then maybe there'd have been way less skeptics.
It's the attitude of the politicians and the mainstream media that created the skeptics.
To me what the mainstream media were publishing about the Covid-19 during the outbreak and the first lockdown was approximately as correct as what they were publishing about SBF/FTX before his ponzi was exposed: a narrative they were fed.
> For it to be a reasonable choice to not want to take the vaccine wouldn't you need to balance the risk of death / complications from the vaccine against the risk of death / complications from covid multiplied by the risk of getting covid?
That would not be a correct comparison, because the vaccine does not prevent you from getting covid. The risks to balance are:
A) The risk of myocarditis and other fatal and non-fatal side-effects from the vaccine, TIMES how many times you get the vaccine, PLUS the cumulative risks of COVID infections over time (which you can get despite being "vaccinated").
B) Just the risks of COVID infections over time.
A is strictly more dangerous than B no matter what the risks of COVID are. Every comment saying, "oh but COVID can cause X risk of death and Y risk of myocarditis and blah blah blah" is completely irrelevant, because all of these risks accrue just as much to the vaccinated. Even if the vaccine is, say, 15% effective, which is very generous given the evidence, then that means that if the risks of the vaccine are 15% as much as the risks of COVID, then (A) is still more dangerous. The risks of the vaccine are more than 15% the risks of COVID, as the evidence is piling up.
Then there's the little fact that the vaccinated are slightly more likely to be reinfected with COVID than the unvaccinated. But the studies on this are still being suppressed, so you can do the math without it and still come up with vaccination being more dangerous for much of the population.
No I don’t need to balance anything based on your criteria. I and I alone decide what goes into my body. Anyone who is scared to walk outside and face hundreds of thousands of pathogens on a daily basis should remain at home. If you want a vaccine, go ahead and get one.
Three things a) we have VAPP now b) polio is not eradicated, check the Global Polio Eradication Initiative website on those. c) in a case where diagnosis was actually improved in the early years of the polio vaccine they discovered they had been dealing with two things with the same symptoms a all along: paralytic polio and Guillean-Barre syndrome. Determining the respective rates of both is an exercise left to the reader.
> but aren't the side-effects of covid well established, on average more severe, and much more common?
You forgot to account for the risk of getting the virus. If you choose to get the vaccine, the probability is 1. But what's the probability of getting Covid? Definitely less than 1.
For certain age groups (young men), the risk of complications * probability of getting the vaccine (1) was more than the risk of complications from COVID * the probability of getting it (let's say 0.25 or so).
Remember, COVID hasn't been shown to be particularly dangerous to young people...
> Remember, COVID hasn't been shown to be particularly dangerous to young people...
Having seen the impact of covid on young family members and others in my extended social circles, I believe that there's a long tail of effects that we won't be able to see the full picture of for years to come. There's a lot more that should be considered in the decision than just risk of death.
Something I've been wondering about: has anybody tried to separate out the effects of the pandemic itself from the symptoms of long covid? So many of the symptoms of long covid are incredibly nonspecific. I believe there was a study on long covid patients that found that the only long covid symptom that had a significant correlation with actually having tested positive for covid was loss of smell and taste. There is a lot of evidence that social isolation and sedentary lifestyles are detrimental to our health and we now live in a world where loads of people barely left the house or spoke to anyone other than their immediate family members for the better part of two years. We're seeing widespread effects throughout society in everything from education to crime to the amount of violent incidents on airplanes. It's likely that millions of people who do not have long covid are currently in some form of mental health crisis related to the pandemic. Overdose deaths and suicides are up. I wonder how many people started the pandemic with no major covid risk factor and now have a risk factor such as obesity or diabetes that can be directly linked to the psychosocial effects of the pandemic.
I'm not suggesting that long covid doesn't exist, but I wonder how much of that long tail of effects can actually be causally linked to covid infection (obviously not talking about things like lung damage, though I do wonder if stress and isolation could have affected previously healthy people's immune systems). My personal experience with mental health issues suggests that they can have severe and wide-ranging physical effects that are as bad as any disease.
I don't have links handy, but I remember seeing studies that show brain aging on the order of ~10 years in long covid patients reporting brain fog. That could also be a result of sedentary living as a result of the lockdown, it seems unlikely that it'd be that severe given the length of time involved.
As far as I know the leading theory is that damage to the circulation systems of some covid patients is causing a reduction in the quality of bloodflow in the brain which has obvious negative impacts on neurons.
I'm a numbers guy. I happened to just stumble onto this article [0], summarizing a study on the vaccines and long covid:
> Compared to an unvaccinated individual, the risk of long Covid in a fully vaccinated individual was cut by only about 15 percent, the study found.
> Dr. Greg Vanichkachorn, director of the Mayo Clinic’s Covid Activity Rehabilitation Program in Rochester, Minnesota, who was not involved with the new study, said the results were not “too surprising.”
> “We know that the majority of folks with long Covid have not had severe infections,” he said.
Not very much help against long covid on average, nothing like the protection against hospitalizations in vulnerable populations.
If you're concerned about an unproven long tail of effects from the virus, you should be equally concerned about the same from the vaccines. They haven't even been around as long as the virus.
> wouldn't you need to balance the risk of death / complications from the vaccine against the risk of death / complications from covid multiplied by the risk of getting covid?
For certain demographics the probability of getting infected might be that low, but at least in every social young adult I know, the risk is averaged to well over 1.0. I've been infected twice, before and after the jab, and in both cases the infection was worse (months of recovery, VO2Max reduction) than the acute vaccine side effects (weekend of feeling shitty). Pre-vaccine I'd say it took around 5 months to fully feel recovered, e.g. able to run a 4-miler without feeling like passing out, where-as post-vaccine and prior infection I was well recovered at the 6-week mark.
Wow that’s so scientific considering those are completely different strains of Covid and one infection you got immune naive and one you got after an infection and a vaccination. It’s so clear as mud
Meanwhile most vaccinated people have had 2-4 shots. Also keep in mind immunity doesn't last forever, so you need to balance the risk of the shot within a certain timeframe versus the risk of Covid times the risk of complications within the same timeframe. You also can't compare the lifetime risk of Covid versus only 1 shot, both occur within a timeframe since immunity from the shot isn't forever.
60% of the population over a 5 month period had detectable levels of antibodies in their blood, so it's at least 60%.
IIRC they are only detectable for a few months (but that maybe also depend on the way of testing I don't know) which would means it's closer to 100% than to 60%.
The risk comparison is indeed not trivial, but I think it's a safe bet that you're going to get covid.
> but that maybe also depend on the way of testing I don't know
There's ~3 possibilities after an infection happens:
* A person's innate immune system quickly fights off the virus. This is a generic set of defenses in our bodies that are always active, and if they succeed then you don't create antibodies in the first place.
* Detectable antibodies, meaning your innate immune system wasn't enough and your adaptive immune system took care of it.
* Antibodies have faded and are no longer detectable. You can still do a T-Cell test (more costly, may take longer?) to find out if you can rapidly create new antibodies, which would mean you're still good despite no longer having antibodies.
There's also the issue of the type of antibodies. The mRNA vaccines are only coding for the spike protein, so your body only learns to fight that - but the virus has mutated away from what's currently in the vaccines. Natural/recovered immunity creates a variety of antibodies that work against different parts of the virus, so that's still effective even against "vaccine escape" variants.
Given there is likely a correlation between behaviors to reduce likelihood of infection (avoiding crowds, properly wearing effective masks) and willingness to get vaccinated, I would wager the odds of catching covid at least once would be elevated among people opposed to vaccination.
COVID is much less dangerous to younger people but there are still very real risks involved, especially non-lethal ones. Assuming a 25% probability of catching it, how are you coming to the conclusion that the risk of the vaccine is higher?
I said within a certain demographic... For old people, the vaccine is obviously worth it. Boys/men from age 10-30, probably not. Hell, a bunch of EU countries literally stopped giving young people the Moderna vaccine:
In addition, ask any young person involved in sports how catching COVID has affected their training and performance. For mostly sedentary people it might feel like catching a bad cold and then recovering. If you're actually consistently pushing your lungs to their max there's definitely long-lasting (maybe not long-term) damage there.
That's actually a perfectly reasonable point. It's a shame you chose such an aggressive tone; as a result, many people will probably dismiss your comment outright.
You forgot to add in the risks of getting COVID and being vaccinated. Every time anyone "does the math" on this somehow they count the vaccine as having 100% efficacy, which is an obvious lie.
Also, if you choose to get the vaccine, then the multiplier for vaccine risks isn't 1, it's 2, or 4, or 6, however many times you get the vaccine.
Yes and it shouldn't just be risk of getting the virus, as it looks like the ability of the virus to migrate to the heart also matters.
With environmental infections, it's possible that most people fight the virus within other parts of the body, with the vaccine it looks like the immune response occurred in the heart for many in this study, specifically right heart, possibly due to proximity or accidental intravascular injection:
>we recorded inflammatory foci predominantly in the right heart, which may suggest a gradual blood-stream derived dilution effect and based on this finding it is at least tempting to speculate that inadvertent intravascular vaccine injection may be contributive
I apologize, when I said your choice of demographic I meant your choice of demographic that encompasses "young" as per the topic of your original comment.
Yes, when including the elderly, cancer and heart disease are greater causes of health-related deaths. Is COVID-19 not the #1 health-related cause of death for "young" people?
> accidents, suicide, drug overdoses and homicide
Not long ago this discussion was about health risks, such as infectious diseases or medical complications. But yes, young people can be pretty reckless.
We were doing arithmetic, such as multiplying the risk of myocarditis and hitherto uncorrelated medical complications by 1.0, and then a number that is likely several orders of magnitude larger (death by COVID, not even the much, much more likely disablement of "long covid") by a number you erroneously claimed was 0.25 and was perhaps around 0.6 almost a year ago (anti-body study, 9/2021-2/2022).
> Remember, COVID hasn't been shown to be particularly dangerous to young people...
I have friends in their early 30s who still haven't recovered their sense of smell. Knoew a 25-year-old who spent 4 weeks with terrible symptoms. I'm a marathon runner and lift and in my early 30s and this disease kicked the shit out of me and had 4 with reduced physical function.
It is very obviously worse than the worst flus almost everyone had and the flu is sufficiently dangerous that it has a nontrivial effect in human quality of life.
> Aren't the side-effects of covid well established, on average more severe, and much more common?
There is no doubt that we'd have a lot more deaths without the vaccines. I suspect that is true for at least some of the lockdowns too.
In my experience, people aren't very good at assessing risks. Actively doing something that comes with a certain risk is often perceived as being more dangerous than passively hoping to avoid what is objectively known to be the greater risk.
If those risks are then contested or associated with a high degree of uncertainty, making an active choice often becomes a question of deferring the decision to someone you really trust. If you don't trust anyone, you're not likely to do anything.
An anecdote - I know a few people who didn't get the vaccine, or got it a lot later than everyone else, and more often than not they have had bad health care experiences in the past. When you've been on the receiving end of one or more mistakes of that kind, it isn't difficult to understand how waiting to see what happens seems like the smarter choice.
I took 3 doses of vaccine but it is no longer effective at preventing infections. Studies that keep coming out show that Covid can have a lot of damaging consequences every time you get infected and they accumulate (https://www.nature.com/articles/s41591-022-02051-3). I have a job and lifestyle that allows me to limit crowded spaces by a lot during wintertime. I will try to avoid getting covid ever again as much as possible, and the vaccine doesn't help much in that. I think the danger from vaccine is very small, but , as in everything, i want to wait a few years before i can trust it.
But to those that plan to get immunized by simply getting Covid again I 'd say "good luck" because they are going to need it
Honest question: why does this matter to you? The vaccine doesn't stop transmission, that's widely acknowledged now, and can't establish herd immunity (unless you plan to vaccinate deer).
It doesn't affect you at all so why waste time thinking about others' cost-benefit analysis?
We all have our reasons. They're all unique and inevitably personal. For my part, standing my ground and resisting the pressure to get jabbed is one of my proudest achievements.
>but aren't the side-effects of covid well established, on average more severe, and much more common?
No they are not well COVID in my view. To me the complications that are supposedly attributed to covid are those of respiratory illnesses that have existed long before COVID came on the scene. In fact I have my doubts whether the whole COVID thing is a brand new disease.
As someone pointed out there are bigger issues: like trust in pharmaceutical companies and current science medical science. In my current view medical science is very primitive, while putting up a front of sophistication and accuracy, while being very crude.
And just so that you know that I'm not a perpetual skeptic, I will go along with Einstein's quotes:
“One thing I have learned in a long life: that all our science, measured against reality, is primitive and childlike -- and yet it is the most precious thing we have.”
Depends on who and when. The idea of vaccinating my young kids in late 2022 is an absurd proposition to me personally - and if the state mandated it, we would leave. This will change once we understand what is happening with these fatalities and correct it.
yeah that's reasonable, and a perfect way to do it is to go by age groups
covid is hurting/killing people who are weak, elderly, and immunocompromised. So covid is the bigger worry here, they should get vaccinated
young kids mostly don't even notice they have covid, and young people in general, ~<30 y/o, don't have any issues from covid. So the vaccine is a bigger risk, and the natural immunity they gain from getting the disease is more advantageous than the vaccine ever would be for their demographic
Im not a skeptic but has to do with the mandate. Has to do with distrust in government, corporations, etc. not fully honest conversations about vaccine etc ..
control group here: I'm doing fine, and have been doing fine all along, just like every single other person I know who is also in the control group. I'm profoundly uninterested in publicly debating my internal decision-making process. though I am interested in hearing from anyone else in the control group to see how they're doing.
Everyone got the vaccine and everyone still got covid. you have to get the vaccine and then covid and then more vaccine and then more Covid and you’re saying it’s clear to you what the benefit risk is in this jumble of vaccinations and Covid vaccines really you know what it is you’re sure you read the paper of the research it’s out there for everyone to just look at?
You are so astoundingly wrong that I'm just glad people like you get coerced into getting vaccinated so society doesn't have to live your terrible risk assessments.
What is your back of the envelope math here? Clearly, the vaccine does not prevent infection. There is no evidence it reduces the incidence of harmful sequelae following infection. So how does this add up to support mandatory vaccination for young men?
Going to be a little hard to credibly show the vaccine protects against infection when everyone is getting infected.
Knowing whether someone is vaccinated against COVID is not going to help you predict whether they have been or will be infected. Knowing whether someone had the smallpox vaccine is going to help you predict whether they had been or would become infected. See the difference?
The risk: benefit analysis that supports vaccination is considering the earliest standards of care we had which were criminally misguided - no steroids allowed, plug patient respiration up with a machine to not spread the virus ,
These protocols are what killed people mostly and ultimately they are what is being used to justify universal recommendations for a vaccine.
We coerced young, low-risk people into receiving these treatments despite known side effects on pain of losing their education or employment or being able to enter privately-owned establishments (irrespective of the wishes of the owners of those privately-owned establishments).
We justified it with the specious argument that they were putting other people at undue risk by remaining unvaccinated. We claimed that vaccinated people would not spread the virus.
And we gave the companies producing these vaccines blanket legal immunity from any potential liability.
We require young people to get vaccinated as a rule in order to obtain education. Every medical intervention involves risks. So does taking a shower or taking the bus to school. We all have to take risks and some of them are mandated for the good of society.
There were very good indications that the vaccine would prevent spread.
Public policy decisions which cost lives are not unusual and although tragic, are often necessary. For instance should we use the entire yearly budget of a hospital to cure one child, or let that child die in order to fund daily operations? These questions have no 'right' answer and no matter what was decided there is going to be criticism and errors which result in less than optimal or even tragic outcomes.
Looking back in hindsight and using the knowledge we now have, I would say that the biggest errors made during the pandemic by public policymakers (besides disbanding the pandemic team and having a leader who was looking at everything in the lens of a what was personally good for him at that moment) was in messaging.
If we can use this to craft a better way to handle public messaging in the future then perhaps we can avoid a lot of the negative societal effects which we are now dealing with -- specifically lack of trust in scientific institutions, division based on ideology and not evidence, and the spread and enabling of conspiratorial thinking.
We generally don't allow parents to force risky irreversible things onto their children. But also, the view of all citizens as simple children of the State seems...problematic.
Conscription is a good example of a social burden unfairly dispersed and widely objected to — at least in the West. My point is the underpinning of this “one more mandatory intervention is no big deal” view is not based on reality. The State stopped forcing irreversible interventions on adults when eugenics went out of (polite) fashion. The belief compulsory acts are normal and good policy is based on something like a public health bureaucracy fantasy version of economics’ perfectly rational actor models.
You make a very good point, but like in times of invasion where conscription is something I would argue is necessary, in times of other emergency then there is the possibility we must give up some independence of our person and perform compulsory acts. This may not be as obvious as getting a needle jabbed into your arm, but rationing water and food, joining in labor to clear wreckage/debris or rebuild, or taking arms in defense during invasion are all examples of similar situations.
I recognize that it is ill-advised to normalize forced medical intervention and I thank you for pointing out that my initial comment appears to be doing that, and I shall make a point to reflect on this, but I do maintain that during times of crisis the state/society should have the right to compel individuals in ways that are otherwise not acceptable.
The problem with that line of thinking, to me, is we have state apparatuses fully and ever-increasingly capable of manufacturing crises to compel individuals in ways that would otherwise not be acceptable. On top of that, I see a qualitative difference between a compulsion of labor or rations impeding bodily autonomy in a superficial sense, and the compulsion of injections (or lobotomies, or sterilization) which seems to strike a deeper and more serious infringement on bodily integrity. Given those factors, I think it's very crucial that societal decisionmakers err towards preserving individual independence and are not misleadingly guided towards other ends.
I see where you are coming from, but I would caution against such comparisons to lobotomies and eugenics. Those interventions were not in response to a large-scale crisis but were novel methods of solving problems for which there had been no previous solution.
I think my comparisons are more apt because they involve sacrifice and risk, but not incontrovertible harm. People getting the vaccine were mitigating a personal risk which at that time happened to be in line with what was believed to be a societal need (herd immunity) -- a minute chance of an adverse effect, compared to the yet-unknown effects of covid itself was deemed to be acceptable.
Was it a poor decision? Looking back on it, yes. If placed in the same position of a society-disrupting and mass-death causing pandemic with a new vaccine which has all the signs of being able to fast-track herd immunity and save millions of lives, would I be fine with mandatory vaccinations? Probably. Should we be incredibly careful when it comes to doing things like that and putting in place the mechanisms for similar actions? Absolutely.
I do not have children so I have no stake in the matter and I do not feel that Id am sufficiently informed about the particulars at this point to have an opinion.
I happened to stumble across this [0], on the effectiveness of a third covid vaccination for 18-29 year olds, while looking for recent (omicron) studies quantifying how well vaccines keep people out of hospitals, and thought I'd pass it along:
> To prevent one COVID-19 hospitalisation over a 6-month period, we estimate that 31207–42836 young adults aged 18–29 years must receive a third mRNA vaccine. Booster mandates in young adults are expected to cause a net harm: per COVID-19 hospitalisation prevented, we anticipate at least 18.5 serious adverse events from mRNA vaccines, including 1.5–4.6 booster-associated myopericarditis cases in males (typically requiring hospitalisation). We also anticipate 1430–4626 cases of grade ≥3 reactogenicity interfering with daily activities (although typically not requiring hospitalisation). University booster mandates are unethical because they: (1) are not based on an updated (Omicron era) stratified risk-benefit assessment for this age group; (2) may result in a net harm to healthy young adults; (3) are not proportionate: expected harms are not outweighed by public health benefits given modest and transient effectiveness of vaccines against transmission; (4) violate the reciprocity principle because serious vaccine-related harms are not reliably compensated due to gaps in vaccine injury schemes; and (5) may result in wider social harms. We consider counterarguments including efforts to increase safety on campus but find these are fraught with limitations and little scientific support.
As an fyi, I also bumped into stats saying that it was something like 5-6 times less likely for vaccinated people to end up in the hospital (although most people who end up in the hospital are elderly), and vaccinations seem to confer only 15% benefit against long covid. I was hoping to find something breaking hopsitalization down by age and comorbidities in addition to vaccination status, but have had no luck so far.
Could you please not fulminate and call names in HN comments? You can make your substantive points without any of that, and it would be in your interest, because comments like this only discredit your viewpoint.
I realize how frustrating it is to hold a minority/contrarian view, but why hand people flaming reasons to dismiss you? All it does is weaken your own position, and you're poisoning the ecosystem by doing it. You can weaken your position if you want to, but it's not ok to poison the ecosystem.
You know what also causes myocarditis? COVID-19 [1].
So the choices were:
1. Don't pressure young people to get vaccinated. Nearly everyone who's unvaccinated eventually catches COVID-19. Some of them would have severe reactions and die; or spend time in a hospital, taking up space and delaying care for others, causing those other people to die. Nearly all of them would pass COVID-19 on to other people, many of whom would be older and die. Some of them would develop myocarditis and die.
2. Pressure young people to be vaccinated for COVID-19. Some of them would develop myocarditis and die.
#2 is strictly better than #1.
Sometimes in life there are no good options; only not-so-great options and very bad options.
That's not necessarily the case, if fact it might be the exact opposite.
1. Don't pressure young people to get the vaccine, some will end up in hospital, some will die.
2. Pressure young people to get the vaccine and 6 times as many of them end up in hospital from the vaccine, taking up more space, and putting more pressure on the system [0], some of them will die [1][2]
One of the cruxes of the issue is what constitutes "pressure". Should we block children from going to school in order to "pressure" them forcing the risk of #1 on them rather than allowing parents to make their own choices?
You still get Covid after you are vaccinated. Fun fact if you are vaccinated before you catch Covid you cannot develop an immunity to the nucleocapsid is this good is this bad I don’t know tune in in 10 years when we know more
As we also coerce babies into screening for various diseaaes and for vax against the diseases that afflict societies without this science. That is how it works. That is why we mostly don't die from infectious diseases for the first time since we built cities.
Not for an emergency use drug that doesn’t maintain herd immunity for a disease that is minimally harmful to children and is under immense selective pressure to break out of the vaccine.
Maybe you’ve got a bad mental model because of the word “vaccine.” This is not a vaccine of the kind we give children, in terms of what it prevents and the extent of data and knowledge we have of its side effects.
This feels like pure revisionism. The purpose of the vaccination programs for children is not to prevent severe disease or death, though that is a nice benefit. The purpose, and manifested effect, is to maintain population herd immunity due to the fact these vaccines radically reduce the chance of the child acting as a vector. The consequence is a vastly reduced incidence rate across the whole population due to this network effect vs a scenario with no mandate. This was widely understood to be the ethical justification for mandating these vaccines: it led to a collective benefit, counterfactually preventing massive suffering across many individual, a benefit which outweighs the risk to the individual from taking these drugs. This fundamental premise is entirely not the case for this vaccine program, which does not come close to helping with herd immunity for a disease we now acknowledge is endemic, and also happens to have a wildly different relative risk profile for children vs the other vaccines we mandate.
You asked for an epidemiologist. I gave you two of the world's foremost practicing infectious disease experts : Rochelle Walensky, MD, MPH, Mass General chief of Infectious Diseases at Massachusetts General Hospital; and Monica Gandhi MD, MPH, Associate Chief of the Division of HIV, Infectious Diseases, and Global Medicine at UCSF.
Fair assumption. But actually I'm Canadian and, while I knew COVID discourse was a clusterfuck in the US, I didn't realize that there were people that clearly knew better blatantly lying about this.
For instance, we KNEW that the best case scenario was 90% effectiveness for the MRNA vaccines. Seeing these people saying "you won't get COVID" is an absolute disgrace and people should lose their jobs and medical certifications for this.
> "I would say 50% would have to get vaccinated before you start to see an impact," Fauci said. "But I would say 75 to 85% would have to get vaccinated if you want to have that blanket of herd immunity."
Months later, May 2021:
Masks off? Fauci confirms ‘extremely low’ risk of transmission, infection for vaccinated
Why should the companies be held liable? This was a government project enforced by the gun; the companies didn't force anyone to take their vaccines, and there's not a way they could have made them meaningfully safer given the timelines.
My employer wouldn't let me go to the office or even any offsites or outdoor actives (i.e. a picnic) until very recently. (Despite my approved religious exemption and "requiring" all employees to work in the office).
If that isn't coercion to take an experimental vaccine i don't know what is.
Seems reasonable to me. They want everyone to be at the office and vaccinated, but they’re not allowed to fire you because “religion”, so they made special accommodations to let you continue working without making all of their other employees have to be around you. You appear to be mad that your “exemption” wasn’t enough to make them pretend you were vaccinated?
> I wouldn't class it as experimental when hundreds of millions of people have taken it.
that just means we're experimenting on hundreds of millions in real time. That was the whole point of the "emergency use".
> your rights versus those of the people you work with
no, employees don't have a legal "right" to work in a fully vaccinated office. That would imply that even if an employer wanted to give someone an exemption, then any employee could veto it.
I would prefer the government was completely indifferent to religious beliefs. Because any belief can be construed as religious if you’re willing to take the position that religion is stupid and you don’t care about optics.
So yeah, I would prefer beliefs not garner you special privileges
What special privileges are being garnered? The topsy-turvy world of the religious person existing as the exception rather than the rule is quite odd to me. But regardless, in the USA the religious exemption policy is incredibly diverse and welcoming, you are correct on that. You do not even need to communicate with your God in expressible ways to other people. What should be the limit on someone's divine communication and the restrictions upon the government they live under?
I would posit that the special privilege has been given to the non-religious, in that they have been able to openly discriminate against religious people in violation of existing laws.
I would suggest looking into the EEOC regulations mentioned by someone else in this thread and Title VII of the 1964 civil rights act.
Is it your position then that it's either your personal belief or a divine communication from your God that the government should be able to discriminate based on religious beliefs, against existing human rights legislation?
I'd prefer that we not all pretend that 2000-year-old religions somehow magically dictated that vaccines were bad. They obviously didn't. These obviously are not legitimate "religious" beliefs. Religion is transparently being used as a cloak for political beliefs fueled by misinformation.
Taking covid-related "religious" beliefs seriously only undercuts societal respect for actual religious belief.
In regards to how religious beliefs are treated in the USA, it's not restricted to the major religions of the world. Someone's communication to their God does not require a many thousand year lineage, it doesn't even need to be able to be communicated in a comprehensible language to others.
It may be that some people aren't professing sincerely held religious beliefs, but if they say they do then as the law is written then it must be respected by their employer. The employer is able to ask some clarifying questions about the religious belief and they only have to provide what would be considered a reasonable accommodation.
The law can certainly be changed but besides the difficulty of the process the implications of allowing the government to gain additional control over what is an acceptable religion sounds like a great way to lead to additional religious pogroms.
> I'd prefer that we not all pretend that 2000-year-old religions somehow magically dictated that vaccines were bad
You don't understand any of the religious arguments if you think its just because it's a vaccine. It could be because fetal tissue was used in manufacturing these vaccines (they were). There are many other such examples.
This is misleading. Some vaccines do use two fetal cell lines in their development or testing. NOT in their "manufacturing". These cell lines were derived from two elective abortions in the 1960s and 1970s. The same cell lines have been used now for over 50 years for various other medical purposes.
Saying "fetal tissue" and "manufacturing" paints rather a different picture.
Also, to be more specific, when we speak of covid vaccines, we're largely talking about the Pfizer and Moderna vaccines. Those specific vaccines did NOT use fetal cell lines in their manufacturing. So now you've gone from being misleading to being flat out wrong.
I understand the pseudo-religious arguments quite well, actually. To that point:
"The Pfizer and Moderna vaccines were found to be ethically uncontroversial by the pro-life policy organization the Charlotte Lozier Institute. Further, the Secretariat of Pro-Life Activities, a committee within the US Conference of Catholic Bishops, has stated: "neither Pfizer nor Moderna used an abortion-derived cell line in the development or production of the vaccine. However, such a cell line was used to test the efficacy of both vaccines. Thus, while neither vaccine is completely free from any use of abortion-derived cell lines, in these two cases the use is very remote from the initial evil of the abortion...one may receive any of the clinically recommended vaccines in good conscience with the assurance that reception of such vaccines does not involve immoral cooperation in abortion."
> Standardized autopsies were performed on 25 persons who had died unexpectedly and within 20 days after anti-SARS-CoV-2 vaccination.
Sample size of 25 out of a population of... how many tens of millions of young (EDIT: not actually young) men? Seems quite small, and perhaps not sufficient to draw any conclusions. I wonder what the results will show...
> myocarditis is another manifestation reported during SARS-CoV-2-infection [24]. It is under debate whether myocarditis in COVID-19 is primarily caused by the viral infection or whether it occurs secondary as a consequence of the host´s immune response, in particular by T-lymphocyte-mediated cytotoxicity or as a consequence of the cytokine storm observed during COVID-19 [25].
Interesting!
> Finally, we cannot provide a definitive functional proof or a direct causal link between vaccination and myocarditis. Further studies and extended registry are needed to identify persons at risk for this potentially fatal AEFI and may be aided by detailed clinical, serological, and molecular analyses which were beyond the scope of this study.
So in total, out of 25 young men, 20 showed signs of cardiac damage. It's suggestive and merits more research. On the other hand, the authors offer no real ideas about how the damage could have happened, other than to observe that since similar damage happens as a result of COVID-19, maybe the immune response is the culprit (provoked by the vaccine, similarly as by the disease).
Far from any sort of smoking gun. It's important to keep that in mind.
>the authors offer no real ideas about how the damage could have happened
They do, though. In fact that's the entirely novel value that this study brings. It's in the title: "histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination." That's a lot of words that means "we can now tell you exactly what microscopic tissue looks like following lethal jab-associated myocarditis.”
And the scientists discuss how it happens. For your benefit, I'll describe it here.
These mRNA-vaccinated patients suffered from heart damage because their hearts were attacked by their own immune cells. The mRNA is injected into your muscle cells, turning the cell into a factory producing COVID-19 spike proteins. As a result of the mRNA immunization, your body generates an immune response against COVID-19 spike proteins. Since your own muscle cells were used to make the COVID-19 spike proteins and may have them on the cell surface, your newly-weaponized immune cells targeting the spike protein may start attacking your own healthy muscle cells. This autoimmune attack on their own heart cells then leads to their damaged hearts beating so many times per second that, once the tachycardia unexpectedly started, they died in minutes.
This new German study shows photographic evidence that this happens and has killed people
> And the scientists discuss how it happens. For your benefit, I'll describe it here.
Condescension noted :)
You've described what I understand to be a common(-ly presented online) hypothesis about how an mRNA vaccine might injure heart tissue. The study authors, on the other hand, don't claim that this is how any of the study subjects died. Indeed they explicitly disclaim any causal link between an mRNA vaccine and incidences of myocarditis.
Allow me to rephrase, then - "the authors offer no real ideas about how the Covid vaccines could have caused this damage".
Fascinating. Without a detailed knowledge of biology, it seems like this could affect any cell type, why would heart muscle cells specifically be targeted? Are the spike proteins just more likely to get stuck to the surface of certain types of cell?
As someone who did choose to get the latest booster despite being a young male (highest risk group for myocarditis I believe), we should always be questioning what we put in our bodies.
I partially agree, or at least think we shouldn't be discouraged from questioning, but there's only so many hours in a day, and a person can digest a finite amount of information.
I choose to trust US health authorities. Flawed as they may be, I think it would be worse to somehow try to verify every claim, or come to my own conclusions on every single question. I won't judge you for making a choice different from my own, but for me, and I suspect many (most?) people, having a doctor who you trust, following their recommendations, and getting on with your life might be the best strategy.
Given the information i had at the time, I am fine with my unforced decision to get the first two doses, but I will not be getting a third barring some surprising new information, new variant, etc.
> we should always be questioning what we put in our bodies
If we did a better job of that, health problems associated with obesity, smoking, drinking, etc... would be reduced and that would have a pretty big impact on cardiovascular health too.
Some are talking about the risk of myocarditis after vaccination as being way less than the risk of dying from COVID. I would say this is just one thing popping up about the vaccines. There no long-term studies of the vaccination even if there are millions and millions of administered vaccines. It's only been three years since the first vaccination was given only 2 years ago, and the control group was burned by giving the placebo group of the control group the vaccine. We don't, and will not know the long-term effects of the vaccine for another 2 to 5 years. The NYT article cited using micromorts to compare this to a soldier in Afghanistan in 2010 is very disingenuous or just bad journalism. It's 12 years after 2010. Let's see where COVID vaccination studies lead to in 2032 for equivalence. Obesity, diabetes, and hypertension were THE amplifiers of COVID deaths, not just COVID. Obesity is the second leading cause of preventable deaths in the US. I contracted COVID pre-vaccine, and having natural immunity ignored completely by the CDC and ruling party, was socially irresponsible. I am speaking of the millions of Americans who had COVID before the vaccine, not people trying to get COVID to get natural immunity. My older children, who also had COVID, were forced by the universities they attended to get vaccinated and boosted. I really hope no long-term effects are found from the vaccine, but I have great distrust of Big Pharma, especially Pfizer. They even burned their control group for a long-term study under the argument they wanted to be humane and vaccinate the placebo group. Yeah, right. Stage 1 for the vaccine's EUA were supposed to include animal biodistribution studies, but even after looking through redacted documents released by Pfizer per the FOIA request to get them, it is not clear. Remember they said it is local to the injection site and breaks down quickly? Let's be prepared to adjust the micromort of the vaccine vs. non-vaccine for people who are not obese, diabetic, or suffer from hypertension and contract COVID in the next 3 to 7 years.
Multiple US universities still mandate the shots for young students in total opposition to Europe, for example: Harvard [0], Yale [1], Tufts University [2], University of California [3], New York University [4], University of Notre Dame [5], Boston University [6]
>>The reported incidence of (epi-)myocarditis after vaccination is low and the risks of hospitalization and death associated with COVID-19 are stated to be greater than the recorded risk associated with COVID-19 vaccination [29].
I hope the research continues to make it even more safe.
When I got second dose of covid pfizer, I remember feeling really strange. My heart was beating really irregularly and I felt like I was struggling to breathe. My vision also started to gray out in a really weird way. I thought I was going to die in that pharmacy for a few minutes. When I snapped out of it, I was covered in sweat
To this day, I don't know if it was a panic attack or a heart attack. Regardless, probably never getting another vaccine after this because just seeing a needle is enough to freak me out
I had the same experience. I will never get a booster. Besides the ten minutes of thinking I was going to die, I ended up getting a severe case of COVID within 60 days of the "vaccine".
These are very low numbers with only 5 vaccine+death cases found in an area with 8mio citizens.
But they convincingly argue that accidentally injecting the vaccination into the bloodstream towards the heart may cause a heart infection similar to those seen in people who got sick with Covid.
Covid-19: politicisation, “corruption,” and suppression of science
"Professor John Ioannidis of Stanford University, quotes an infection fatality rate (IFR) for Covid of 0.00-0.57% (0.05% for under 70s), far lower than originally feared and no different to severe flu" -March 2020
The fatality rate for a disease that is very often asymptomatic highly depends on testing. The rate will go way down in places where lots of people are required to or just do get treated frequently.
Most asymptomatic cases will go unnoticed in places with less testing so the fatality rate will go way up.
Also how you count whether or not a death gets tagged with covid matters. Lots of people had Covid and plenty of deaths will just coincidentally happen while a person has a minor infection which didn’t affect the outcome. How or when do you count that?
A survey by the most cited epidemiologist alive is not a forecast for one. It is the best appeal to authority one can make. I've seen it shown that h1n1 in england in 2009 had a IFR of 0.05% which is greater than the revised figure for covid.
Amazing how all the proof in the world makes such little difference to the average Luddite who will just defer to authority regardless. Stanley Milgram was clearly right about everything he said.
The vast majority of cases are mild, yes. This doesn’t change the fact that Ionnadis’ predictions of the severity of the pandemic were off by a factor of x100.
Here is a pretty good recap of his blundering walk through covid
>"The overall incidence of myopericarditis from 22 studies (405 272 721 vaccine doses) was 33·3 cases (95% CI 15·3–72·6) per million vaccine doses, and did not differ significantly between people who received COVID-19 vaccines (18·2 [10·9–30·3], 11 studies [395 361 933 doses], high certainty) and those who received non-COVID-19 vaccines (56·0 [10·7–293·7], 11 studies [9 910 788 doses], moderate certainty, p=0·20). Compared with COVID-19 vaccination, the incidence of myopericarditis was significantly higher following smallpox vaccinations (132·1 [81·3–214·6], p<0·0001) but was not significantly different after influenza vaccinations (1·3 [0·0–884·1], p=0·43) or in studies reporting on various other non-smallpox vaccinations (57·0 [1·1–3036·6], p=0·58). Among people who received COVID-19 vaccines, the incidence of myopericarditis was significantly higher in males (vs females), in people younger than 30 years (vs 30 years or older), after receiving an mRNA vaccine (vs non-mRNA vaccine), and after a second dose of vaccine (vs a first or third dose)."
Regardless of any possible danger of vaccination, one has to also consider that vaccination doesnt prevent infection, which is important. As more studies come to light it s becoming evident that Covid damages our bodies in many ways, even with mild infections, it weakens our immune systems and the damage is cumulative every time we catch it. We should be preventing infections , with measures that are appropriate, instead of trying to mitigate the symptoms as we do with vaccines.
> Of note, it has been recently reported that intravenous injection of COVID-19 mRNA vaccine is able to induce an acute (epi-) myocarditis in a preclinical model
There have been lots of vaccinations shown in various TV reports over the last years. Watching carefully, there's two different variants: a) jab, aspirate, inject, b) jab, inject. Maybe it is just stock footage and not from covid shots, and everyone has been checking carefully for not finding blood?
Small sample size (n = 25), small number of incidents of myocarditis, no causal link found between myocarditis and adverse events (including, but not limited to, death) and no causal link found between mRNA vaccines and myocarditis.
But do you what does cause myocarditis? Getting Covid [1].
Covid and the (highly effective) vaccines are the most clearcut case of evolution in action [2] I've seen in my lifetime.
This isn't really worth worrying about this point. Countries (barring China) have largely decided they're over Covid. Get a vaccine, don't get a vaccine. Nobody cares. Looking for justification for not getting a vaccine however reminds me of creationists trying to equate "intelligent design" as "science".
We knew this over a year ago, but it's called "acceptable risk" by the CDC. The thing is they never told us that. But it was on that document you signed when you took your jab.
You read the fine print right?
Moderna had "This is an EXPERIMENTAL VACCINE" on all thier media until not that long ago, and then they just removed that warning. We don't even have clinical trials any more.
Those Moderna shareholders are rough, once a week jab was the goal. That booster. Much upset there, when that did not go through.
They tried to push "your dog, cats, all your pets WILL need a shot!" That did not get much traction, remember that news?
Shareholders bailed. Lets all short TSLA was their next move. How markets work.
What most of you still supporting "vaccine" failed to understand is that a jab cannot be developed in less that 1 year. It was a huge experiment and many people paid with either their lives or have suffered severe damage. All for a virus that kill less that common influenza, which a much more dangerous corona virus than covid.
Actually, the vaccine was developed relatively quickly. The testing and ramp-up is what took the vast majority of time.
You're sort of following the pre operation warp speed statements that the press and "experts" were spouting before they actually did it.
But now there are vaccines for covid that are made in the standard fashion. It took them longer to get out of the gate, but they're around. Not sure if they're in the US, though.
There is no law of nature that says a vaccine cannot be made in a year, in the same way that there is no law of nature forbidding any of our technological artifacts that we use every day.
Influenza is not a coronavirus.
Influenza does not kill anywhere near as much as the original SARS-CoV-2 strain.
And mortality was not the only concern regarding the pandemic.
It never had before, because a commercial mRNA vaccine had never been the right trade off of immunity vs development time.
Until COVID-19 there had not been a pandemic we needed to address with a vaccine since mRNA vaccination tech became widespread several decades ago. If we had enough time to develop a vaccine, why sell a new one that doesn’t work as well as the old kind?
The discussion here is absolutely rancid. So here are the actual the salient points from the study:
> Standardized autopsies were performed on 25 persons who had died unexpectedly and within 20 days after anti-SARS-CoV-2 vaccination. In four patients who received a mRNA vaccination, we identified acute (epi-)myocarditis without detection of another significant disease or health constellation that may have caused an unexpected death.
Out of 25 people that died post-vaccination, four patients had signs of myocarditis. That's a fraction of a fraction of people.
> Myocarditis is another manifestation reported during SARS-CoV-2-infection [24]. It is under debate whether myocarditis in COVID-19 is primarily caused by the viral infection or whether it occurs secondary as a consequence of the host´s immune response, in particular by T-lymphocyte-mediated cytotoxicity or as a consequence of the cytokine storm observed during COVID-19
We don't know whether or not Myocarditis is a result of the infection or the immune response; in either scenario people who are predisposed to myocarditis would likely have similar reactions during either infection or vaccine.
> However, the vaccine against smallpox, based on a vaccinia virus, is reported to cause (epi-)myocarditis in rare cases
Smallpox vaccines can also trigger myocarditis despite being a more 'traditional' vaccine.
> The reported incidence of (epi-)myocarditis after vaccination is low and the risks of hospitalization and death associated with COVID-19 are stated to be greater than the recorded risk associated with COVID-19 vaccination [29]. Importantly, infectious agents may also cause lymphocytic myocarditis with a similar immunophenotype, thus meticulous molecular analyses is required in all cases of potentially vaccination-associated myocarditis.
The risk factor is low and the chances of hospitalization and death from COVID-19 in even otherwise healthy people is higher versus the risk from vaccination, similar to other vaccinations.
> Finally, we cannot provide a definitive functional proof or a direct causal link between vaccination and myocarditis. Further studies and extended registry are needed to identify persons at risk for this potentially fatal AEFI and may be aided by detailed clinical, serological, and molecular analyses which were beyond the scope of this study.
This is not a definitive link between the two, but rather a call for further investigation and to ensure that at-risk individuals are caught earlier and monitored.
We don't know whether or not Myocarditis is a result of the infection or the immune response; in either scenario people who are predisposed to myocarditis would likely have similar reactions during either infection or vaccine.
This is the most straightforward conclusion. Some people’s hearts don’t like the immune response to Covid. Since everyone is going to get it eventually, avoiding the vax seems based on myocarditis seems illogical.
It seems obvious at this point that there is a mechanism of action of the drug in the vaccine that can harm the heart and it’s highly likely this can lead to death. It’s time to stop mandating it for kids.
Obvious according to who? I literally directly addressed that claim, so I'll quote it again for you:
> Myocarditis is another manifestation reported during SARS-CoV-2-infection [24]. It is under debate whether myocarditis in COVID-19 is primarily caused by the viral infection or whether it occurs secondary as a consequence of the host´s immune response, in particular by T-lymphocyte-mediated cytotoxicity or as a consequence of the cytokine storm observed during COVID-19
We don't know whether or not Myocarditis is a result of the infection or the immune response; in either scenario people who are predisposed to myocarditis would likely have similar reactions during either infection or vaccine.
If myocarditis is a result of the immune system response to the spike protein then infection by COVID and/or vaccination can potentially trigger a response, with COVID likely triggering an even worse response with what we know and how it travels through the body. Additionally, as I also mentioned and will quote:
> However, the vaccine against smallpox, based on a vaccinia virus, is reported to cause (epi-)myocarditis in rare cases
Smallpox vaccines can also trigger myocarditis despite being a more 'traditional' vaccine.
We distributed smallpox vaccines and managed to eradicate smallpox thanks to being thorough.
The claim I am making is it appears likely to me that at least some of these cases are fatal, which would mean the underlying mechanism of action for this side effect of the drug can, in the worst case, cause death. This ought to influence the ethics of mandating it at a minimum.
What I'm saying is that the mechanism with which the vaccine can cause myocarditis might be the exact same mechanism that triggers myocarditis but worse for people who catch COVID-19, as brought up in the study. If the myocarditis is the result of the immune system's response to the spike protein then both COVID-19 and the COVID-19 vaccine will trigger myocarditis in those individuals. In this case the 'mechanism' is the same, but COVID-19 will likely trigger a far worse reaction from what we know about how the disease progresses in certain individuals.
This is the exact point that the article mentions.
So the argument is that if the vaccine causes this the same way COVID does, the risk of death would have been higher had they got COVID?
You’ll have to excuse my skepticism, because setting things up so that we end up in a situation where it’s entirely unfalsifiable if the vaccine caused net harm in an individual has been par for the course. I reject the premise that even if it’s an immunological response shared by with COVID we should run with that to the assumption that catching COVID would have yielded a higher risk profile. That takes a far leap ahead of the science.
We literally know COVID yields a higher risk profile for myocarditis. This data has been well captured through multiple studies. And that's just solely on the basis of myocarditis and not the other side effects we're also aware of like the damage to lung tissue, blood clotting and more.
To provide an allegory, you are trying to point of the incidence rate of myocarditis in the smallpox vaccine and claiming that the smallpox vaccine was more dangerous than smallpox itself.
You’re smuggling in the assumption that the vaccine induced myocarditis is the same underlying phenomenon, with the same risk profile, as the viral induced one.
Let’s say, hypothetically, that what was going on here was some % of vaccines were being injected intravenously in error, leading to massively localized spike protein buildup in the heart over a few hour period, with dynamics highly divergent with the progressive, broad way it would run with actual disease, causing a different set of possible outcomes like instant death being very much on the table. In this hypothetical scenario, can you see why your analysis about immunological response being similar, and myocarditis being caused by the disease and vaccine being relevant, would turn out to have in fact been missing the point? And that by failing to do so, we missed a simple protocol change that could have saved many lives counterfactually?
I’m not saying that is what is going on. But what I am saying is if that scenario is logically coherent to you, can you extrapolate why the kinds of responses you are giving here could be falling into the the same trap you’d have recognized if the above scenario was actually what was happening? You’re telling me that I should stop thinking something bad is going on here, that we can stop, and am making nonsense arguments like the one you raised with the smallpox vaccine. I reject that - this is important and we should figure it out.
Believe your own eyes and ears. The raw data became completely useless once the federal government gave hospitals a blank check for particular codes and treatments.
People will believe whatever they want to believe.
They only found 5 deaths that had no other real issue besides the vaccine. At that level more people died from shower accidents than vacccine-induced myocarditis (assuming that there was a causal link, which the authors are careful to say they didn't do that analysis).
Interesting, but I'd need far more medical knowledge than I have to put this into context. Does this mean people with existing heart conditions should avoid these vaccinations? Does it mean those at otherwise very low risk for severe COVID-19 shouldn't bother? I sure dunno.
Myocarditis is rare and has been a part of the discussion from even before the vaccines were released, or at least the professional discussion. They were why the vaccines were not recommended for all ages to begin with.
In absolute terms, yes. But relative to other vaccines, it's much more common.
I also read that the chances are like 1 in a million per dose (not the right number, you get the point) but since its per dose your chances are actually like 1 in 40,000 after 3-4 doses.
The vaccines were and still are mandated for people not at risk of severe disease, and myocarditis has been framed as a side effect not worth worrying about despite the fact that it literally can kill you. Not to mention without understanding the mechanism of action, we cannot estimate the number of true deaths that occurred without a myocarditis diagnosis.
> Besides pneumonia, myocarditis is another manifestation reported during SARS-CoV-2-infection [24].
I mean, your point only makes sense if you ignore that COVID causes the same myocarditis and ignore that the vaccine has been proven to reduce severity and duration of symptoms. This study was of 5 autopsies, unless you can prove this was incredibly widespread concern I don't understand why you think it would be better people get COVID.
On a slightly different note I find it incredibly funny how the refrain was "they died with COVID, not from", but now it's "they died because of the vaccine, not with".
The data on myocarditis has been clear and significant for quite some time: 1 in approximately 5000 young men under 40 by shot two. Without a full understanding of the underlying mechanism of action, we can’t be that confident of number of deaths due to the vaccine, but given the size of the deployed population and the recurrent nature of the shots it’s not unreasonable to think we killed tens of thousands of people with them.
> it’s not unreasonable to think we killed tens of thousands of people with them.
It's not unreasonable to think otherwise as well given that it was a rare occurrence and typically mild. Also, there were no young men in this study. "Median age at death was 58 years (range 46–75 years)", so you're drawing your own conclusions without data here.
I’m not drawing conclusions - you invented that claim. The data I’m referring to is available in several other studies, with regards to estimated myocarditis rates in young men. But if you agree with me that it’s not unreasonable to think that is the scope of fatalities, I would urge you to integrate that new prior into things like the ethics of mandating this drug for college.
Saying it’s not unreasonable means there is some significant probability that we may ultimately determine this to be the case. The conclusion is about the range of probabilities, not the actual state of reality. But probabilities matter when you are deploying policies like mandating kids take this drug to go to college.
You already implies you agree with my claim about it not being unreasonable when you said “as well.” I guess you retract that?
And again: this study is just one of many studies that have lead to my prior. The rate of myocarditis is well established, the population size is well established, the open question is the fatality rate. The unreasonable part comes from putting a lower bound on the death rate based on some assumptions around these studies which have done autopsies and the estimates on subclinical heart interactions from the drug. There are several studies on all of these things. The back of the napkin math to me is on the order of tens of thousands of unnecessary deaths.
> You already implies you agree with my claim about it not being unreasonable when you said “as well.” I guess you retract that?
Yes, I was trying to show polite respect for your point and not actually endorse it, but to be clear, I don't believe there is enough evidence to assume that tens of thousands of young people died, especially not with this article, and especially when you consider that the acknowledged gap in your knowledge is the fatality rate.
Anything that gets your immune system going can trigger an autoimmune crisis, including, you guessed it viruses - which also use RNA to cause your cells to produce spike proteins, by the way.
We can estimate from excess death statistics that this is basically a non-risk for most people. Unlike getting ill with COVID, which we can also estimate from excess death statistics is a notable risk factor for most people.
Young people were at extremely low risk from covid. It is entirely possible that the vaccine killed more people than it saved under a certain age. It is not certain but it is plausible as the covid deaths for young people were so low.
> about despite the fact that it literally can kill you.
There are many many things that can literally kill you. Heck, even anosmia can literally kill you under the right circumstances.
What matters is the total number of vaccine-related myocarditis cases, and the total number of vaccine-related myocarditis death balanced with the number of covid related-death (including Covid-induced fatal myocarditis, because the virus itself has this effect), that's how you get a cost-benefit analysis.
False, the idea that pure net deaths is the only way to think about all that happened is the common thread that people have been clinging to for far too long. It is time to wake up, and remember principles of bioethics, the risk of authoritarian coercive forces, and the nature of dehumanization campaigns. You do not mandate rapidly formulated, under-tested, frontier technology emergency drugs for all humans to work and live especially once there is evidence they may have a consistent mechanism of action that can cause sudden death, and especially once you learn the risk from the disease is highly dependent upon demographics and other comorbitities in a way risk from this side effect isn’t.
Sorry to annoy you with the basics of public health policy.
And the cost-benefit analysis being different for different age classes and comorbidity is exactly the reason why the vaccines was slowly expanded to larger demographics after starting with the most vulnerable people.
In fact, the side effects of the vaccine have been much more thoroughly tracked than many pollutants that are routinely introduced in everybody's life and which somehow never trigger such a reaction from you others who care so much about all this when it comes to vaccines. The amount of hazardous material that are being put in everything from food to cosmetics or kids' toys is appalling, but all you guys have to complain about is vaccines… You claim to care about under-tested frontier technology, but somehow aren't bothered with sunscreen or bisphenol S, why is that?
I'm not part of any "guys", I'm not part of a tribe that you are imagining. I'm just someone who is vaccinated and thinks the mandates violate all traditional bioethical norms given what we have known for a while: the drug is experimental, under studied (no long term phase IV data), does not lead to herd immunity, has a novel mechanism, has a known serious side effect in 1 in 5k or so young men, and the risk of COVID is low in children, and there is a very real danger we are causing large scale subclinical heart damage to children by administering this drug so widely.
In other words, it should not be mandatory.
Public health policy is not entirely about risk vs reward - it's also a branch of medicine, and people who practice medicine have a code of ethics. Everyone acknowledges the risk vs reward choice is in favor of getting vaccinated for almost everyone. But it's a canard at this point, and is being used to gloss over an immense amount of truly horrible stuff that happened during the vaccination campaign of 2021.
> I'm not part of any "guys", I'm not part of a tribe that you are imagining.
Your comment history says otherwise.
> thinks the mandates violate all traditional bioethical norms
Mandatory vaccination has been the norm in many developed countries since at least the polio vaccine…
> there is a very real danger we are causing large scale subclinical heart damage to children by administering this drug so widely. In other words, it should not be mandatory.
But in what country is the vaccine mandatory for children again?
> and is being used to gloss over an immense amount of truly horrible stuff that happened during the vaccination campaign of 2021.
But you won't tell what this very «truly horrible stuff» is, will you? And what was the purpose of the conspiracy according to you? Big pharma making money? (why give vaccines then, when remdesivir is 3 orders of magnitude more expensive than the vaccine?) Or more fancy hypothesis like 5G tracking chips or masse sterilization of white population to replace them with immigrants?
I know of a few people who have opted to not get the vaccine. One lost his wife. Still not vaccinated. You might need some more qualifiers for the word "mandated."
The US executive branch attempted to make it so that your unvaccinated friend had to choose between taking the vaccine or being able to work at most companies.
I agree, it'll probably be scrubbed from the frontpage shortly. It's sad that this is the case, especially since it's published in a scientific journal.
I think you're jumping the gun a bit here. If vaccines save 10,000 people and kill 10 people, that's still a net positive. That's the kind of moral calculus public health has to deal with all the time.
I’m not jumping the gun - the net deaths can be negative yet it is still the case that what we witnessed was a massive, arguably unprecedented failure of medical ethics, the defense of body autonomy, the scientific process, the culture of healthy skepticism and debate, and basic decency and opposition to dehumanization campaigns. All due to fear and righteousness, as it often is.
If the numbers come out that net deaths are sharply negative, do you think we should similarly condemn those that spread fear and misinformation about the safety and efficacy of the vaccine? Or are "skeptics" immune from repercussions for their actions in this case?
The former group has been condemned, banned, ostracized, and dehumanized. To the degree any of them were acting on bad faith or in violation of their oaths, yes they should be condemned.
But the deepest crimes lie elsewhere, by those in power who coerced others into taking drugs they did not want, who used ends-justify-the-means reasoning to violate ethics as physicians or public health officials, and who now continue to try to suppress, deflect, and gaslight us from recognizing the real events which actually occurred and which we are morally obligated to correct for our children.
Agree to disagree, I guess. I'd rather give the benefit of the doubt to those acting on the best information available at the time rather than "influencers" raising "concerns" based on nothing but their gut instincts.
Or to put it another way, how many vaccine skeptics were pushing for the heavy use of masks, better HVAC systems in buildings, and social distancing when possible? Because I've noticed a large correlation between those that spoke out against vaccines and those that spoke out against any preventative measures at all - regardless of how benign.
You’re just cherry picking - there have been plenty of people raising basic concerns about the bioethics of mandating an emergency use medicine using a new technology for a rapidly evolving respiratory virus. There have also been prominent public officials saying things like “the unvaccinated cannot be trusted.” You should not let tribalism get in the way of seeing the full picture of what happened.
Did their stances actually contribute to public health policy, if so then they bare responsibility unfortunately. Armchair biosecurity advocates should be left off the hook.
I would agree with klipt: why were so many influential figures allowed to spread disinformation based apparently on misunderstanding mathematics, the scientific process, and just caring about general health and welfare?
It was said once that 5 deaths is a tragedy, but 500k is just a statistic (as a justification of genocide). This is possibly why the 5 deaths in the article possibly from the vaccine is apparently more terrifying.
For 1.5 years we had the notion of "1 death is 1 too many" shoved down our throats at every turn to justify some pretty heinous encroachments on personal freedom.
I never said that any mitigation was unnecessary. There is a such thing as going overboard. There are still outdoor areas that are closed off despite there being no credible cases of outdoor transmission. https://www.latimes.com/projects/california-coronavirus-case...
If what you are saying is true, then the whole mechanism of https://en.wikipedia.org/wiki/Humoral_immunity is not working. So the human body maintains a complete system that produces useless antibodies?
What he is saying is not true. The large vaccine trials have always been about testing the effectiveness at combating disease directly (measuring rates of reported illness or hospitalization), with antibody titers used as a quick secondary check. His comment assumes the reverse happened. We still know surprisingly little about how long antibodies are measurable in the blood and for how long and how effective they are at what prevalence rate, etc.
Yes but does the government have the ability to coerce or force you to do something with a '1 in 1000' death rate, if not, what is the number we are allowing in the name of public health.
I really do believe myocarditis is an issue with the mRNA vaccines, but how can you claim both "Many died" and "First we need an accurate death count"? How do you know many died if there is not an accurate count?
> We find evidence in support of discriminatory attitudes against the unvaccinated in [nineteen different countries including the US]
> Findings suggest that...the vaccinated react with discriminatory attitudes against...the unvaccinated. Elites and the vaccinated general public appealed to moral obligations to increase COVID-19 vaccine uptake but the present findings suggest that discriminatory attitudes including support for the removal of fundamental rights simultaneously emerged
In the USA on a government level? No idea, at least it isn't a thing around where I live, but I also sit at home and get paid to write software. No idea what applying for jobs in some industries might look like.
On the social level? People have fractured families over it and/or forced(you can't see your grand children unless you're vaxxed, for example)/coerced family members into getting it despite their otherwise refusal. I still know people who won't let non vaccinated people come over for events. It's a much rarer thing now, but the damage has been done.
Yep. I'm now estranged from half my extended family because of the awful way they treated my unvaccinated brother. They invited him to visit for Thanksgiving, knowing he was unvaccinated and saying it was okay. Then after he drove 8 hours to visit, they changed their mind and wouldn't let him into their house. They gave him a sandwich and told him to eat it on the porch. They're dead to me after that.
But wait 15 minutes to see if your child gets anaphylaxis from them. We could have tested for allergy before giving the vaccine but its more convenient to have you wait around after.
Don't worry if you experience allergic shock we have epinephrine on standby. It might not work and its use is associated with Alzheimer's onset but don't worry! Safe and effective!
"But wait 15 minutes to see if your child gets anaphylaxis from them. We could have tested for allergy before giving the vaccine but its more convenient to have you wait around after."
The waiting period of 15 minutes after a vaccine has always been recommended. It's standard medical recommendation and safety.
These type of complaints has actually been really enlightening for me regarding how many people can't even be bothered to get the flu vaccine or their tetanus shots.
I got a tetanus shot a year ago and they didn't ask me to wait around afterwards. They just handed me the paperwork and showed me the door (this was after they had already stitched me up.)
I see the CDC website says that a 15 minute wait after getting a tetanus shot is recommended due to a fainting risk. But I bet this is not widely observed. I surmise they had already judged me to not be a fainting risk, since I didn't faint when they were sewing me.
The CDC discusses anaphylaxis as a possible side effect of the tetanus shot too[1]. It would seem the difference between the two is an adherence to protocol as opposed to risk profiles.
According to the CDC the rate of anaphylaxis is incredibly low with the COVID shot[2].
VAERS includes thousands of reports of death including broad anaphylaxis following their vaccination for CV. So what are you saying? Those lives are an acceptable cost for the convenience of skipping failsafes?
You're essentially giving full confidence to an industry - so why stop at covid? Shouldn't you prophylactically vaccinate yourself against all the viruses on earth?
What this article does describe, is how the fatal "adverse events" take place. It's useful to deepen our understanding of the mechanisms of action for undesireable outcomes. And of course it's one piece of a much larger puzzle.
Some seem to be interpreting this article as a confirmation that vaccines are inherently not safe. The thing is, every therapy, whether preventative or curative carries an element of risk. This paper is not weighing on the relative safety of the immunization.
To someone uncomfortable with the vaccine, this is of course unsettling to discuss, as it reinforces a fear. It's akin to discussing how exactly people's organs got smashed when they got killed by getting ran over by a bus. People who distrust busses will further cement their fears about them.
{kind=link}
{kind=link}
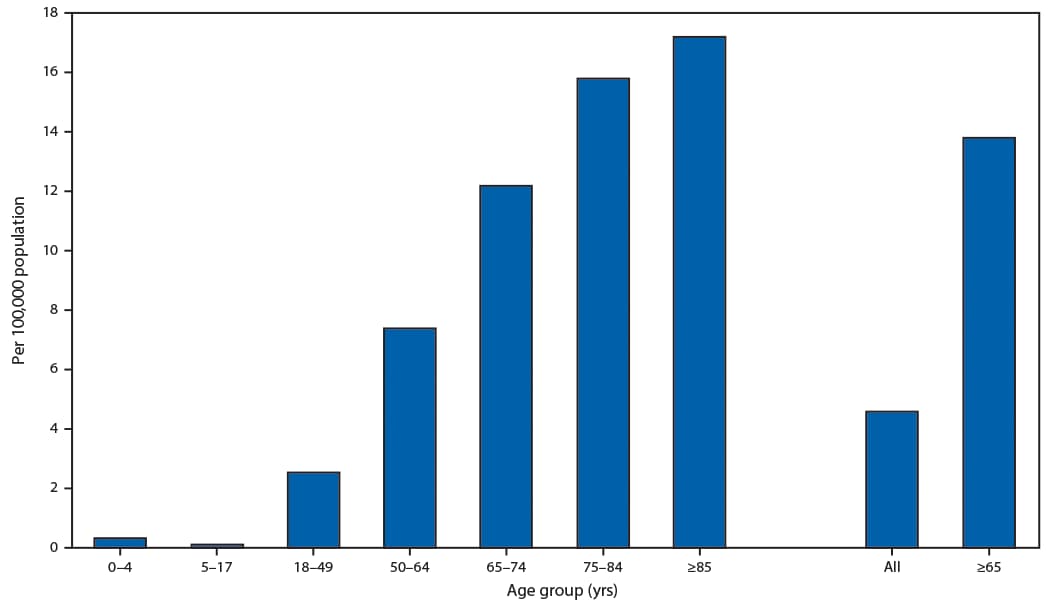{kind=link}
Currently, I still believe that people should vaccinate, even if vaccines cause mortality/harm in some cases. As long as vaccine side effects cause less deaths and less harm than the virus, vaccination is still the way to go.
My position depends on us having a good understanding of the vaccine's effects however, and right now I feel like we don't.